


STANDARDIZATION OF CERVICAL VESTIBULAR EVOKED MYOGENIC POTENTIAL TESTS WITH AIR AND BONE CONDUCTION STIMULATION IN HEALTHY ADULTS
Summary
Objective: The aim of this study was to obtain normative data on Cervical Vestibular Evoked Myogenic Potentials (cVEMP) test in adult age group to use as a differential diagnostic test in our clinic.Materials and Methods: This prospective study was conducted on 50 volunteers who were completely healthy, had no history of vestibular disorder and hearing loss, and had normal otoscopic and audiologic examination results at the Department of Ear-Nose-Throat. The p13 and n23 latency, p13-n23 interpeak latency and p13-n23 amplitude values of both ears of the subjects in the study were analyzed.
Results: In the examination of mean values of cVEMP with air and bone conduction sound stimulation according to the genders, there was a statistically significant difference in the comparison of air conduction p13 latency, n23 latency and p13-n23 amplitude and bone conduction p13 latency (p <0.05).
The air and bone conduction cVEMP test according to age groups was evaluated; a statistically significant difference was calculated according to the age groups in p13-n23 interpeak latency air conduction measurement and p13 and n23 latency bone conduction measurement values (p <0.05).
Conclusion: In addition to the determination of normative values of our clinic in this study, we hope to make a contribution to the studies conducted on this matter in the literature through the results of the present study. Additionally, limit values of cVEMP test parameters assessed in the present study were also calculated. Determination of these values would be able to enable to form our standards to establish differential diagnosis of various diseases in the future.
Introduction
Balance is maintained by perceiving the proprioceptive, visual and vestibular stimuli correctly and quickly and by developing the most suitable motor response [1]. Sensory inputs, integration mechanisms, and disruptions in the end organs cause dizziness and imbalance in the patient. The fact that the symptoms are often non-specific and there are many diseases in the differential diagnosis makes it difficult to identify the cause of dizziness [2]. The first thing to be done for a patient applying with the complaint of dizziness is to determine the complaint correctly. Thus, vestibular system evaluation is started by taking the detailed history and continued with a full neurootological examination. In order to determine the localization of the pathologies causing the complaints of these patients, several test methods and radiological evaluations are required. The presence of the difficulties in the application of some tests have led the physicians to search for new, easy, simple, and non-invasive test methods in order to evaluate the vestibular system.The responses obtained in the Cervical Vestibular Evoked Myogenic Potentials (cVEMP) test, that is first described by Colebatch [3], evaluate the saccular and inferior vestibular nerve different from other conventional clinical vestibular tests [4]. While passing of the reflex arc of cVEMP via the saccular and inferior vestibular nerve enables this test to be specific for the determination of the location of the lesion, and also to be become widely used in clinics as a complementary test in other vestibular tests, today [5]. According to the normative values determined in the cVEMP tests performed in normal children and adults, differential diagnosis of some pathological conditions of the vestibular system can be made and also they can be used in the diagnosis of some central pathologies. However, every clinic should perform a test standardization and obtain normative data. The results obtained from the standardization studies performed in different clinics will provide maximization in practice for clinicians and will be a common ground for the evaluation of VEMP findings in terms of differential diagnosis [6].
The aim of this study was to obtain normative data on cVEMP test with air and bone conduction stimulation in adult age group to use as a differential diagnostic test in our clinic.
Methods
Study PopulationThis prospective study was conducted on 50 volunteers (100 ears in total) in 18-60 age group who were completely healthy, had no history of vestibular disorder and hearing loss, and had normal otoscopic and audiologic examination results at the Department of Ear-Nose-Throat (ENT), Sivas Cumhuriyet University. In the study, 100 ears of 50 healthy individuals in the age range of 18-60 years (25 (50%) men and 25 (50%) women) were evaluated. The individuals were grouped in 4 age ranges as 18-29, 30-39, 40-49 and 50-60. The number of subjects to be included in the subject group was determined by a statistical evaluation by taking the number of cases in similar studies in the literature as a basis [6-8].
All the volunteers participating in the study were informed by the researchers and then their oral and written consents and consent form were taken. Ethics approval of this study was obtained from Sivas Cumhuriyet University Clinical Trials Ethics Committee (dated 03.08.2017 with decision no. 2017-08/04) and it was also accepted by ???UBAP (Sivas Cumhuriyet University Scientific Research Projects (Project no: T-754).
After complete ENT examinations of the volunteers were made, audiological examinations and positional tests were performed. All the cases were subjected to audiological examination and cranial nerves examinations. Then, after performing finger-nose test, past-pointing test, and dysdiadokinesia among the cerebellar tests, Romberg test, Unterberger test and walking test among the postural tests were applied. Following the assessment of the vestibulo-ocular reflex, dix-hallpike maneuver and lateral canal test, that are the most commonly used positional tests, were applied. As a result of the otologic examinations, individuals with average pure tone hearing threshold better than 20 dB and with no nystagmus detected in positional tests were included in the study.
In the study, systemic diseases, recurring diseases related to the ear or active ear infection, air-bone gap more than 10 dB at 500-4000 Hz, limitation in eye movements, anatomic disorder in external ear, anatomic disorder or skin disease that inhibit the localization of the electrodes to be attached around the neck during the test, previous surgeries related to the ear or neck and/or audiovestibular disease (imbalance and/or dizziness), previous malignancy, syphilis, the status of receiving chemotherapy and radiotherapy, presence of congenital cochlear malformation, use of ototoxic drugs, positive history of serious head or ear trauma causing sequala, and otologic, neurologic, cardiovascular, psychiatric, orthopedic, and ophthalmologic diseases that may be specified among the reason of dizziness were accepted as exclusion criteria. In addition, we excluded cases where we could not provide full cooperation in terms of test position in order not to affect the reliability of our results.
Test procedure
cVEMP examination was performed by a GN otometrics ICS CHARTR EP 200 (Natus Medical, Taastrup, Denmark) device from right and left SCM"s to all the individuals. In order to get cVEMP"s, the patient should contract the sternocleidomastoid (SCM) muscle. Lifting the head in the lying position or turning the head sideways in the sitting position is the mostly accepted method for activating the SCM muscle [7]. Before cVEMP, all the volunteers were informed about the procedure to be applied in detail and then they were requested to be in the sitting position in a quiet room and to turn their heads in contralateral direction of the stimulant and to preserve this position throughout the test period. Thus, the contraction of SCM muscle of the stimulated side was provided.
In the study, Ag/AgCI surface electrode (Ambu Blue Sensor N ref No N-00-S/25; Medisave UK Ltd, Weymouth, UK) was used. In the literature, there are studies pointing out that the responses obtained in cVEMP test may vary depending on different electrode localization [9,10]. The electrode layout of the studies in the literature was taken as a basis in order to obtain the best amplitudes and latencies in the cVEMP test and in the present study, the active electrode was placed in the 1/3 middle section of the SCM muscle, the negative electrode in the middle of the opposite SCM muscle, and the earth electrode on the forehead [9-11]. During the test, it was paid attention that the electrode impedance was below 5000 ohms. Stimulations were given monaurally to the right and left ears, respectively and a delay period of 0.80 ms was considered [12]. Firstly, a sound stimulation was given via an insert earphone in order to get the records of cVEMP with air conduction sound stimulation and the records were taken from contralateral SCM. After this tests procedure was completed, a bone conduction sound stimulation was given and a sound stimulation with 50 dB intensity was given by a B71 stimulator on both right and left mastoid bones and again, the same records were taken from contralateral SCM.
When 500 Hz tone burst was used, p13-n23 wave morphology was obtained more significantly, thus in the present study, 500 Hz tone burst stimulus was used and the behaviours were compared [13,14]. It was determined that filter was 10Hz-1KHz and averaging number was 250. Recording was done from a single channel and starting from 105 dB nHL, the intensity was decreased by 5 dB and the thresholds were detected. In order to check the accuracy of the responses obtained from the patients, cVEMP responses obtained by the same waveform and latency in minimum two consecutive tests were evaluated. Via the presence of the first positive p13 and the following negative n23 waves, it was accepted that the individuals had a cVEMP response. The p13 and n23 latency, p13-n23 interpeak latency and p13-n23 amplitude values of both right and left ears of the subjects in the study were analyzed [15].
Statistical Analysis
"Statistical Package for Social Sciences (SPSS) 23.0" statistical package program was used for statistical assessment. For the test of normality, Kolmogorov Smirnov test was applied. In the assessment of the mean values of groups, Wilcoxon rank test and Mann Whitney U test were used for non-parametric variables and dependent/independent samples t test was used for the parametric variables. The relationship of age with latency and the amplitude values was evaluated by Spearman correlation analysis. p value less than 0.05 was accepted as significant.
Results
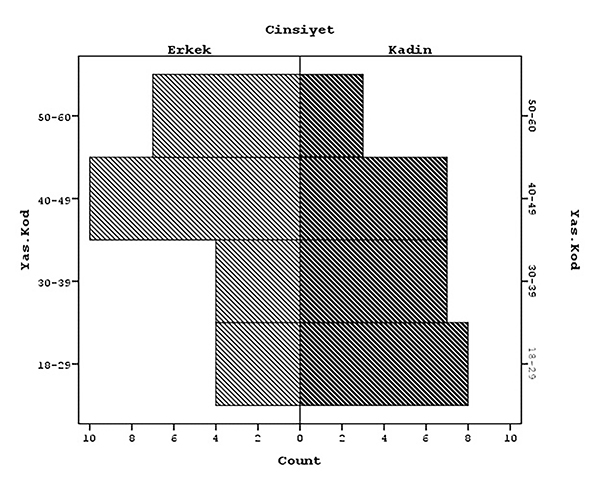
Demographic Characteristics of the CasesThe mean age of the male cases included in the study was 43.8±11.76 years, and the mean age of the female cases was 36.44±12.39 years. Graphic 1 shows distribution of the individuals according to the age and gender and there was no statistically significant difference between the groups (p>0.05; p=0.233).
 Büyütmek İçin Tıklayın |
Graphic 1: Distribution of genders according to the age groups |
cVEMP Assessment
VEMP responses up to 90 dB nHL were obtained in all the cases included in the study. During the VEMP application, the thresholds of the cases were determined. VEMP thresholds of all the cases was observed up to 90 dB nHL.
Air and Bone Conduction cVEMP values for both ears
Kolmogorov and Smirnov test was used whether or not p13 and n23 latency, p13-n23 interpeak latency, and p13-n23 amplitude measurement values of both right and left ears were normally distributed in the evaluation of cVEMP with air and bone conduction. It was observed that the results obtained other than left ear p13-n23 amplitude and right ear p13 latency for cVEMP with air conduction stimulation and left ear p13 latency and p13-n23 interpeak latency for cVEMP with bone conduction stimulation were normally distributed. (Graphic 2).
 Büyütmek İçin Tıklayın |
Graphic 2: The ones excluded from the normal distribution among the test parameters assessed a) Normality examination of left ear air conduction cVEMP p13-n23 amplitude values; b) Normality examination of right ear air conduction cVEMP p13 latency values; c) Normality examination of left ear bone conduction cVEMP p13 latency values; d) Normality examination of the left ear bone conduction cVEMP p13-n23 interpeak latency values |
Table 1 shows the mean cVEMP values with the air and bone conduction sound stimulation obtained from a total of 100 ears evaluated in the study.
){kind=link}
Table 1: Average values of cVEMP executed by air and bone conduction stimulation
There was no statistically significant difference in the latency, amplitude and interpeak latency values according to the ear side tested (p> 0.05).
Air and Bone Conduction cVEMP values for both genders
In the examination of mean values of cVEMP with air and bone conduction sound stimulation according to the genders, there was a statistically significant difference in the comparison of air conduction p13 latency, n23 latency and p13-n23 amplitude (p<0.05). This difference was due to longer p13 and n23 latencies in female and higher p13-n23 amplitudes in male. Similarly, there was a statistically significant difference in bone conduction p13 latency measurement according to the gender (p <0.05). And this difference was due to longer p13 latency in female. (Table 2).
){kind=link}
When the measurement parameters were assessed according to gender and ear side, the results are shown in Table 3. In the evaluation made according to the tested ear side and gender; a statistically significant difference was observed in n23 latency and p13-n23 amplitude in the right ear and in p13 amplitude in the left ear in air conduction cVEMP and in p13 latency values in the right and left ears in bone conduction cVEMP (p <0.05).
){kind=link}
The Relationship of Age with Air and Bone Conduction cVEMP Findings
When assessing statistically the age-dependent change in test parameters in air conduction cVEMP evaluation, it was observed that p13-n23 interpeak latency values would shorten with the probability of 35.6% in the left ear and the probability of 32.7% in the right ear with increasing age (p=0.006, z=-0,356; p=0.010, z=-0,327; p<0.05, respectively). On the other hand, in bone conduction cVEMP assessment, it was observed that p13 latency values would statistically significantly shorten with the probability of 26.5% in the right ear and 37.6% in the left ear and n23 latency values would shorten statistically significantly with the probability of 27.7 in the left ear and 28.8% in the right ear (p=0.031, z=-0,265; p=0.004, z=-0,376; p=0.026, z=-0,277; p=0.021, z=-0,288; p<0.05, respectively). No correlation was observed between other parameters assessed and age (p>0.05).
When the change in the measurement values of the parameters obtained from the air and bone conduction cVEMP test according to age groups was evaluated; a statistically significant difference was calculated according to the age groups in p13-n23 interpeak latency air conduction measurement and p13 and n23 latency bone conduction measurement values (p <0.05). This difference was caused by the shortening of the interpeak latency value as of > 30 years; bone conduction p13 latency value as of > 40 years, and n23 latency value as of > 50 years (Table 4).
){kind=link}
Table 4: Change of the air and bone conduction cVEMP findings of the cases according to the age
Comparison of Bone and Air Conduction cVEMP Values of the Study Group
When the values of the cVEMP with air and bone conduction stimulation were compared, it was observed that in bone conduction, p13 latency values were longer, p13-n23 interpeak latency values were shorter in both ears and amplitude values were lower in the left ear and these differences were statistically significant (Table 5).
){kind=link}
Table 5: Comparison of the values of cVEMP with air and bone conduction stimulation
General assessment
In order to determine the normal standard intervals of cVEMP test parameters of our clinic, the limits related to the values in the study were calculated. The values of 90% and higher were calculated in order to accept cVEMP values of the cases in the sample group as a basis and establish differential diagnosis of diseases by using these standards in patients to be assessed in the future. Accordingly, Table 6 shows the right and left ear rates within ±2 SD for every measurement value.
){kind=link}
Table 6: Percentage values of the ears within ±2 SD for each one of cVEMP measurement values
Discussion
Dizziness and imbalance constitute a major problem in general public health. The reasons of dizziness may vary from self-limiting disorders to life-threatening disorders. There are various test methods used in the subjective and objective assessment of the vestibular system. Combined application of these tests and assessment of the results provide important information for the clinicans in order to make the correct diagnosis and effective treatment of the patient.Historically, the oldest vestibular test method is caloric test. In this test method, vestibulo-ocular reflex (VOR) is assessed through the horizontal semicircular canal. Similarly, in the electronystagmography and videonystagmography tests, eye movements generated by various stimuli are recorded and VOR pathways are functionally evaluated. In the head impulse test, being a new test method, all of the six semicircular canals are evaluated. Different from these tests, the function of otolith organs in the VEMP test is important for showing the superior and inferior vestibular nerve, otolith-ocular and otolith-cervical reflexes. This test method is generally used in clinical practice in order to determine the normal functioning of saccule, inferior vestibular nerve and central connections and it plays an important role in the differential diagnosis of many pathologies such as semicircular canal dehiscence, Meniere's disease, benign paroxysmal positional vertigo, vestibular neuronitis, and acoustic neurinoma [6].
In recent years, VEMP has been increasingly used as a diagnostic test in many clinics. However, each clinic should also obtain its own normative values for this test. It should not be forgotten that normative data is obtained to facilitate general clinical use and that meta-analysis studies comparing these data are needed [16]. In the present study, we aimed to determine normative values of cVEMP responses in healthy adults for our clinic and to provide both use them as normative data in future studies and use effectively this test method in differential diagnosis of various vestibular system diseases.
In various studies performed for VEMP applications; application parameters, localizations of electrodes and the study findings differ from each other. In order to use any test in differential diagnosis, application and evaluation parameters should be standard and sufficient data for normal population should be collected. Since the results obtained with VEMP testing performed within certain standards can allow for obtaining important results in diagnosis of various pathologies, we paid attention that the used test parameters had similar standards with the studies in the literature as far as possible in order to increase reliability of the present study"s results and use the results in many different studies.
The amplitudes of the waves obtained in cVEMP vary from a few millivolts to several hundred millivolts depending on muscle tension and the stimulus intensity. Amplitudes show a wide distribution even in the studies conducted with healthy individuals. Thus, there is no consensus for the minimum value of cVEMP amplitudes in the literature [3,17]. In the study conducted by Lee et al., [18] on 97 healthy cases, they determined the average amplitude as 17.0 ± 7.3?V (5.9-47.2 ?V) in 194 ears; on the other hand, Tulğar et al., [17] found the average amplitude as 19.7 ± 7.7 (6.5 ? 40.4) ?V. In the present study, the air conduction amplitude rate was found as 43.79±11.59 (9.05- 74.42) ?V and the bone conduction amplitude rate was found as 41.55±6.86 (19.85- 57.52) ?V, and although the average values were higher than other studies, they were similar to the other studies when the wide distribution interval was considered.
Although latencies vary according to the type of stimulus and age, they are more stable than the amplitude. Therefore, average values of p13 and n23 latency and p13-n23 intervals are assessed for comparison in most of the cVEMP-related publications. Isaradisaikul et al., [19] assessed 50 healthy volunteers in order to compare both the results obtained from cVEMP with air conduction stimulation and their protocols with results of the studies investigating other normative values in the literature. They found no statistically significant difference between the right and left ears in terms of the parameters evaluated in the study. Similarly, in the studies of Tulğar et al., [17], Lee et al., [18] and Trivelli et al., [20], it was observed that there was no statistically significant difference between the two ears in the evaluation of air conduction cVEMP. In the present study, we observed no statistically difference between the right and left ears in terms of p13 latencies, n23 latencies, p13-n23 interpeak latencies and amplitudes in air and bone conduction cVEMP tests of 50 right and 50 left ears, which is compatible with the literature.
In the cVEMP test, many studies have revealed that there is no significant difference in the analysis of p13 and n23 latency values according to the genders [17,18,21-23]. However, in some of the studies, it is pointed out that the mean values of latency and amplitude may vary according to gender. For example, in the study by Felipe et al., [21], no significant difference was found in terms of wave latencies compared to genders, whereas the amplitude value was found to be significantly higher in men than women. In the present study, mean amplitude values in the assessment of cVEMP with air conduction sound stimulation were higher in male patients than female subjects. Various studies in the literature also point out that higher amplitude values in males than females may be caused by the degree of muscle contraction of the amplitude [24,25]. However, different from the study of Felipe et al., [21], p13 and n23 wave latencies in air conduction cVEMP test and average p13 patency in bone conduction are found to be longer in female cases than in male cases in the present study.
In the study by Carnaúba et al., [22], the ear side was also included in the assessment besides the genders, and when the cVEMP results were evaluated, no statistically significant difference was observed between the genders and the test parameters assessed with the ear side-gender. The study by Tulğar et al., [17] pointed out that there was a statistically significant difference between p1 and n1 latency values of female and male cases; however, they found that this difference was statistically insignificant when Eta square test was applied. In the present study, the results obtained upon the comparison of both right-left ear area and female-male genders showed that right ear n23 latency and left ear p13 latency in air conduction cVEMP assessment as well as right ear and left ear p13 latency values in the bone conduction according to ear direction and gender showed a statistically significant difference. The results of the present study were similar with the results of Tulğar et al.[17] when the numerical parameters were taken as a basis. Consequently, various studies in the literature observed no correlation between gender and cVEMP test parameters. We thought that the difference observed in the present study was associated with the fact that the cases could not contract SCM muscle equally at both sides. We think that if muscle tensions are provided to be equal with more sensitive measurements, this difference can be eliminated, thus they can be consistent with the results in the literature. In order to make a contribution to the reliability of our results, we suggest that planning of a detailed study will be useful by considering the contraction grade of SCM muscle in the future.
Emergence of various morphologic changes in the vestibular system is inevitable depending on aging. Therefore, it is inevitable to monitor various changes in the VEMP parameters caused by the effects of aging. Thus, it is important to consider the age of the patient while interpreting the VEMP responses of the individuals. The most consistent finding of the aging effects on VEMP parameters is the decrease in amplitude values with the increasing age. Some studies revealed that latency values prolonged with increasing age. However, the results of the studies investigating the differences between age-related cVEMP values in the studies in the literature show differences from each other. The most important reason for this is the fact that in most of the studies, the level of contraction activity of the SCM muscle is monitored visually and a direct comparison is generally not possible due to the failure to make a specific standard assessment [26-28]. As a result, there is no consensus in the literature regarding the effect of the age on p13 and n23 latencies [13,18,28,29]. This is caused by two reasons. The first reason is that exact origin point of p13 and n23 waves is not known [18]. The second reason is that even though aging affects everyone, there are individual differences in degrees in its effect. In the study by Tourtillott et al. [26], since there was no statistically significant difference in cVEMP parameters evaluated in the left-right ears and gender categories, assessment was performed by taking the mean value of the ears for every patient and combining the gender data in every age category for all the other analyses. As a result of this assessment, cVEMP amplitudes had a statistically significant difference among the age groups and the amplitude values decreased significantly in the age group of 75-85 years. In addition, the result of the present study indicating that there was no statistically significant difference in the evaluation of latency measurements related to age was shared with the literature. In the study by Felipe et al., [21], it was observed that the aging in saccule did not lead to changes in VEMP parameters in single cases older than 60 years. Differently from the study by Tourtillott et al., [26]; in the present study it was determined that while no significant change was observed in the amplitude values, a statistically significant difference was observed in p13-n23 interpeak latency air conduction measurement, p13 and n23 latency bone conduction measurement values according to the age groups; and this difference was caused by showing a shortening of the interpeak latency value as of >30 years old; bone conduction p13 latency value as of >40 years old, and n23 latency value as of >50 years old. The results of the present study are different from those of other studies in the literature and we think that this is the natural result of dependence of the correlation between age and cVEMP parameters on several variables.
Conclusion
In conclusion, in accordance with the aim of our study, normative data of cVEMP test were obtained for the healthy adult age individuals in our clinic. Additionally, limit values of cVEMP test parameters assessed in the present study were also calculated. Determination of these values would be able to enable to form our standards to establish differential diagnosis of various diseases in the future. Also we believe that publishing and evaluating the results of studies conducted in different clinics aiming to obtain normative data in order to use cVEMP findings as a differential diagnostic tool will contribute to the literature.Sources of support in the form of grants: Sivas Cumhuriyet University Scientific Research Projects (Project no: T-754).
Conflict of Interest: The authors have no conflicts of interest to declare.
Financial disclosure: The authors declared that this study has received financial support from YYY UBAP.
Reference
1) Welgampola MS, Colebatch JG. Charasteristics and clinical applications of vestibular evoked myogenic potentials. Neurology 2005; 64: 1682-1688. [ Özet ]
2) Ardıç FN. Vertigo. Özdek A. Öyküye dayalı ayırıcı tanı yaklaşımı. İzmir. US Akademi. 2019: (7); 69-75.
3) Colebatch JG, Halmagyi GM, Skuse NF. Myogenic potentials generated by a click-evoked vestibulocollic reflex. J Neurol Neurosurg Psychiatry 1994; 57:190-197. [ Özet ]
4) Wang CT, Young YH. Earlier And Later Components Of Tone-Burst Evoked Myogenic Potentials. Hear Res 2004;191(1-2):59-66. [ Özet ]
5) Rosengren SM, Welgampola MS, Colebatch JG. Vestibular evoked myogenic potentials: Past, present and future. Clin Neurophysiol 2010;121(5):636-51. [ Özet ]
6) Derinsu U,Baş Eİ, Akdaş F. Vestibüler uyarılmış miyojenik potansiyellerin standardizasyonu. Marmara Medical Journal 2009;22(2);127-133.
7) Fu XX, Liu B, Qi BE, Ji C, Guan JZ. [Characteristics of cervical vestibular evoked myogenic potential in different test positions]. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2016; 51(9): 650-654. [ Özet ](Abstract)
8) Meyer N, Vinck B, Heinze B. cVEMPs: a systematic review and meta-analysis. IntJ Audiol. 2015; 54(3): 143-51. [ Özet ]
9) Colebatch JG. Mapping the vestibular evoked myogenic potential (VEMP). J Vestib Res. 2012; 22(1): 27-32. [ Özet ]
10) Sheykholeslami K, Murofushi T, Kaga K. The effect of sternocleidomastoid electrode location on vestibular evoked myogenic potential. Auris Nasus Larynx. 2001; 28(1): 41-3. [ Özet ]
11) Papathanasiou ES, Murofushi T, Akin FW, Colebatch JG. International guidelines for the clinical application of cervical vestibular Evoked myogenic potentials: An expert consensus report. Clinical Neurophysiology Journal. 2014; 125(4): 658-666. [ Özet ]
12) Wang, S.J, Young, YH. Vestibular evoked myogenic potentials using simultaneous binaural acoustic stimulation. Hearing Research. 2003; 185(1): 43-48. [ Özet ]
13) Janky KL, Shepard N. Vestibular evoked myogenic potential (VEMP) testing: Normative threshold response curves and effects of age. Journal of the American Academy of Audiology. 2009; 20(8): 514. [ Özet ]
14) Maes L, Vinck BM, De Vel E, D?haenens W, Bockstael A, Keppler H, Swinnen F, Dhooge I. The vestibular evoked myogenic potential: A test?retest reliability study. Clinical Neurophysiology. 2009; 120(3): 594-600. [ Özet ]
15) Cal R, Bahmad F. Vestibular evoked myogenic potentials: An overview. Brazilian Journal Otorhinolaryngology. 2009; 75(3): 456-62. [ Özet ]
16) Driscoll C, Bekessy A, Bui V, Fox D, Harvey M, Mackenzie D. Vestibular evoked myogenic potentials: Clinical implications of a normative investigation. Aust NZ J Audiol 2007; 29:98-112.
17) Tulğar M, Özdek A, Bayır Ö, Saylam G, Tatar E, Korkmaz MH. Normal işitmeye sahip kişilerde logon stimulus kullanılarak yapılan servikal vestibüler uyarılmış miyojenik potansiyel (VEMP) ölçümü. KBB-Forum 2012:11(4);81-6. [ 18) Lee SK, Cha CI, Jung TS, Park DC, Yeo SG. Age-Related Differences in Parameters Of Vestibular Evoked Myogenic Potentials Acta Oto-Laryngologica. 2008; 128: 66-72. [ Özet ]
19) Isaradisaikul S, Navacharoen N, Hanprasertpong C, Kangsanarak J. Cervical vestibular-evoked myogenic potentials: norms and protocols. Int J Otolaryngol. 2012; 2012: 913515. doi: 10.1155/2012/913515. [ Özet ]
20) Trivelli M, Vicini C, D'Ascanio L, Greco F, Salvinelli F. The effects of logon versus click on vestibular evoked myogenic potentials. Acta Otolaryngol 2008;128:314-317. [ Özet ]
21) Felipe L, Santos MA, Gonçalves DU. Vestibular evoked myogenic potential (Vemp): evaluation of responses in normal subjects. Pro Fono. 2008; 20(4): 249-54. [ Özet ]
22) Carnaúba AT, Farias VV, Santos N, Oliveira AC, Rodrigues RG, Menezes Pde L. Influence of gender on the vestibular evoked myogenic potential. Braz J Otorhinolaryngol. 2011; 77(2): 245-8. [ Özet ]
23) Basta D, Todt I, Ernst A. Normative data for P1/N1-latencies of vestibular evoked myogenic potentials induced by air- or bone-conducted tone burst. Clin Neurophysiol 2005; 116: 2216-9. [ Özet ]
24) Sheean GL, Lim CL, Yiannikas C. Some non- pathological variables affecting the vestibular evoked potential. Aust NZJ Med. 1993;23:572.
25) Lim CL, Clouston P, Sheean G, Yiannikos C. The influence of voluntary EMG activity and click intensity on the vestibular click evoked myogenic potential. Muscle Nerve. 1995;18(10):1210-3. [ Özet ]
26) Tourtillott BM, Ferraro JA, Ahmed AB, Almquist E. Age-Related Changes in Vestibular Evoked Myogenic Potentials Using a Modified Blood Pressure Manometer Feedback Method. American Journal of Audiology. 2010: 19;100?108. [ Özet ]
27) Ochi K, Ohashi T. Age-related changes in the vestibular-evoked myogenic potentials. Otolaryngol Head Neck Surg. 2003; 129(6): 655-9. [ Özet ]
28) Su HC, Huang TW, Young YH, Cheng PW. Aging effect on vestibular Evoked myogenic potential. Otol Neurotol. 2004; 25(6): 977-80. [ Özet ]
29) Welgampola MS, Colebatch JG. Vestibulocollic reflexes: normal values and the effect of age. Clin Neurophysiol. 2001; 112(11): 1971-9. [ Özet ] ![]() Tam Metin ]
Tam Metin ]