


ASSOCIATION BETWEEN VERTIGO AND CEREBRAL LATERAL VENTRICULAR ASYMMETRY DETECTED ON COMPUTED TOMOGRAPHY AND MAGNETIC RESONANCE IMAGING
2İstanbul Okan Üniversitesi Hastanesi, Radyoloji Anabilim Dalı, İstanbul, Turkey
3İstanbul Okan Üniversitesi Tıp Fakültesi, Tıp Fakültesi, İstanbul, Turkey
Summary
Objective: To determine the association between vertigo and lateral ventricular asymmetry (LVA) detected on computed tomography (CT) and magnetic resonance imaging (MRI).Materials and Methods: In a tertiary center, the cranial CT and MRI scans performed between December 2016 and April 2018 were evaluated by a radiologist. The scans that had LVA with any pathology were excluded and those without any pathology were included. Patients who had LVA were contacted over the phone and asked if they had vertigo at the time of the imaging. Patients who had vertigo were asked to answer the Vertigo, Dizziness, Imbalance (VDI) questionnaire over the phone. LVA was classified by the radiologist into grades I, II, and III.
Results: Of the 689 CT and 1018 MRI scans, LVA was detected on 62 (8.9%) and 85 (8.3%), respectively. The mean age was 36.13±12.53, and 50.34% of the patients were women. Of the 83 patients who responded over the phone, 33 (39.7%) had vertigo at the time of the imaging. The mean VDI score was 46.74±11.79. There was a statistically significant and positive linear correlation between age and the LVA grade (p=0.008). The VDI scores were significantly lower in women compared to men, which implies that vertigo is worse in women with LVA (p=0.009).
Conclusion: Vertigo occurs in patients with LVA, and more commonly in women. Age is a factor influencing the LVA grade, but this grade has no influence on vertigo symptoms.
Introduction
Lateral ventricular asymmetry (LVA) is a common radiological finding with an uncertain etiology, and the incidence is 5-12% [1]. LVA is often considered a nonspecific radiological finding, except in cases of space occupying lesions, intracranial bleeding, recent infarction, and trauma [2,3]. LVA may be associated with neurodegenerative diseases, Parkinson's disease (PD), and left- or right-handedness [4]. Mechanisms underlying LVA have been hypothesized. The basal ganglia and thalamus surrounding the lateral ventricles are affected by PD, which might be a reasonable explanation of the association between LVA and PD [5]. However, the limits of acceptable LVA have not been established [2].Vertigo is a sensation of loss of balance and can be a symptom of either central or peripheral vestibular disorders. Central vestibular disorders may produce sudden vertigo and more prolonged symptoms that last up to several weeks. Classically, the central and peripheral causes of vertigo have been differentiated based on the duration of vertigo attacks: episodic or constant. Although constant vertigo is associated with a central cause, many central processes also produce episodic vertigo, especially in the early stages [6].
The purpose of this study was to evaluate the association of LVA with vertigo symptoms.
Methods
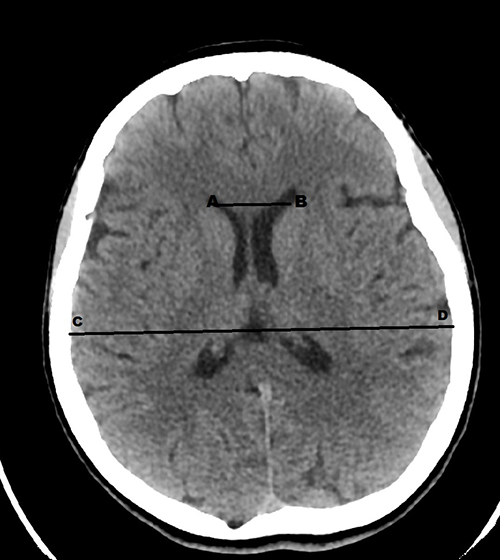
This study was approved by the Institutional Review Board of the Maltepe University. A retrospective review of 689 cases of computed tomography (CT) and 1018 cases of magnetic resonance imaging (MRI) of the head was performed, including patients referred to radiology department between December 2016 and April 2018. The exclusion criteria were CT or MRI findings of space-occupying lesions, intracranial bleeding, recent infarction, trauma, and postoperative scanning. The remaining scans were evaluated by one radiologist for LVA, and those with LVA were enrolled in the study. The patients (1707) had undergone axial scanning (CT or MRI) of the brain using the equipment manufactured by the GE Healthcare. CT was performed with the GE Optima series, with a slice thickness of 0.625 mm. MRI was performed with the GE Signa 1.5 Tesla series, with a slice thickness of 5 mm. The sagittal T2-weighted, sagittal T1-weighted fluid-attenuated inversion recovery (FLAIR), axial T2-weighted FLAIR, axial T1-weighted FLAIR, and axial T1-weighted fat-suppressed MRIs were used.The Evans' index [7] is the ratio of the maximum width of the frontal horns of the lateral ventricles and the maximum internal diameter of the skull at the same level on axial CT and MRI. A score of less than 0.3 is considered normal, but it can be higher for the elderly individuals. The diameter of each horn was measured electronically at the level of the head of the caudate nucleus, and the measurements were used to evaluate the degree of LVA (Figure 1). The smaller size was divided by the larger diameter to produce the ratio of LVA, with a ratio of 1-2:1 indicating grade I, 2-3:1 indicating grade II, and >3:1 indicating grade III LVA.
 Büyütmek İçin Tıklayın |
Figure 1: The Evans" index: AB/CD (used in grading of the lateral ventricular asymmetry) |
Patients with LVA were contacted over the phone and asked if they had vertigo at the time of the imaging. Patients with vertigo were asked to answer questions, over the phone, from the vertigo symptom scale component of the Vertigo, Dizziness, Imbalance (VDI) questionnaire [8]. This questionnaire measures vertigo symptoms on a scale and their effect on the quality of life. The questionnaire was the Turkish version of the inventory, which consists of 36 items. It has been translated to Turkish and proven reliable and valid [8]. The inventory has two components: vertigo symptom scale (14 questions) and quality of life (22 questions). The inventory asks respondents about the frequency of certain sensations associated with their symptoms. Each item consists of a 6-point rating scale ranging from 0 (all the time) to 5 (never). Subsequently, each of the two components provide a sub-score, with the maximum score being 70 and 110 for the first and second components, respectively. A high score indicates few vertigo symptoms and high quality of life [8]. Only the vertigo symptom scale was evaluated for the patients over the phone in this study.
Statistical analyses were performed by the jamovi project (2018). The jamovi computer software version 0.9.0.3 was used (https://www.jamovi.org). A p-value equal to or less than 0.05 was considered statistically significant. The independent-samples t-test, Mann?Whitney U test, and Kruskal?Wallis H test were used depending on the distribution of the digital variable.
Results
Of the 689 CT and 1018 MRI scans, LVA was detected on 62 (8.9%) and 85 (8.3%), respectively. A total of 147 patients had LVA (42.18%, CT; 57.82%, MRI). The mean age was 36.13±12.53, and 49.66% of the patients were men, while 50.34% were women. Of the 83 patients who responded over the phone, 33 (39.7%) had vertigo at the time of the imaging and answered the VDI questionnaire. The mean score of VDI was 46.74±11.79. The ventricle was hypertrophied on the right and left sides in 47.62% and 52.38% patients, respectively. The mean LVA grade was 2.19±0.63'tür. The number of patients with grades I, II, III was 18 (12.2%), 82 (55.7%), and 47 (31.9%) respectively. The number of patients with grades I, II, and III who responded over the phone was 10, 47, and 26, respectively. The percentage of patients with grades I, II, and III who had vertigo was 10% (n=1), 36% (n=17), and 53.8% (n=14), respectively. There was a positive correlation between the LVA grade and presence of vertigo. Patients with vertigo were asked if they had positional vertigo. Positional vertigo was not present in 51.61% of the patients, while right and left lateralization were present in 19.35% and 29.03% of the patients, respectively. The VDI scores had no statistically significant correlation with the side of ventricular hypertrophy on CT or MRI (p >0.05) or the LVA grade (CT: p=0.39; MRI: p=0.8; CT+MRI: p=0.44). There was no statistically significant correlation between gender and the LVA grade. However, there was a statistically significant and positive linear correlation between age and the LVA grade (p=0.008). The VDI scores were significantly lower in women compared to men, which implies that the vertigo symptoms were worse in women with LVA (p=0.009).Discussion
LVA is often considered a nonspecific anatomical structure and has not been well analyzed. LVA can be caused by space-occupying lesions, recent infarction, trauma, or intracranial bleeding, but without a cause, this finding on CT or MRI could be interpreted as an anatomical variant [2]. Changes in the surrounding structures may contribute to ventricular hypertrophy, such as a decreased volume of the hippocampus, caudate, putamen, thalamus, or cortex in PD patients [9?11], while some studies did not find any differences [12,13]. LVA has been associated with some neuropsychiatric diseases, such as attention deficits, infantile autism, language disorders, Tourette syndrome, schizophrenia, and anorexia nervosa [2]. Harcherik et al. found LVA in 13% of the autism, 22% of the language disorder, 9% of the attention deficit disorder, and 16% of the Tourette syndrome patients [14]. Possible pathophysiological association between any of these diseases and LVA is unknown.Kiroglu et al. compared 170 head CT with LVA and 170 head CT without LVA in clinical characteristics and found that headache was statistically significant in patients with LVA, but there was no statistically significant correlation in vertigo [2].
Dizziness and vertigo can be caused by diverse pathological conditions of the central nervous system. Classically, the central and peripheral causes of vertigo are differentiated based on the duration of vertigo attacks: episodic or constant. However, occasionally, central and peripheral causes can occur simultaneously. Migraine and motion sickness are thrice more common in patients with benign paroxysmal positional vertigo, which is the most common type of peripheral vertigo, compared to the general population. Additionally, the frequent co-occurrence of Meniere's disease, which can cause peripheral vertigo, and migraine suggests an association between the two syndromes. Alternatively, the diseases may be separate processes that cause similar symptoms [15]. Thus, many things remain unknown. LVA has not been well-analyzed, and there could be an association with vertigo, as 39.7% of the patients with LVA who responded over the phone had vertigo in our study. Although our study has several limitations that restrict the generalizability of the findings, this percentage is considerable with sufficient screening number of subjects. There are many causes of vertigo in the clinical practice, and thus it is hard to show a strong association of vertigo and LVA depending on our survey results. Our study had a retrospective design, and we could only question the patients over the phone. Moreover, there was no control group. Still; in the lights of our results, future prospective studies with more diagnostic techniques may enlighten this commonly seen imaging-finding in the everyday practice.
Reference
1) Grossman H, Stein M, Perrin RC, Gray R, St Louis EL. Computed tomography and lateral ventricular asymmetry: clinical and brain structural correlates. Can Assoc Radiol J. 1990; 6:342-346. [ Özet ]
2) Kiroglu Y, Karabulut N, Oncel C, Yagci B, Sabir N, Ozdemir B. Cerebral lateral ventricular asymmetry on CT: how much asymmetry is representing pathology? Surg Radiol Anat. 2008; 30:249-255. [ Özet ]
3) Lewis MM, Smith AB, Styner M, Hongbin G, Roxanne P, Hongtu Z, et al. Asymmetrical lateral ventricular enlargement in Parkinson's disease. Eur J Neurol. 2009; 14: 475-481. [ Özet ]
4) Cha S, George AE. How much asymmetry should be considered normal variation or within normal range in asymmetrical frontal horns of the lateral ventricles noted during CT brains scans without evidence of midline shift or any other significant lesion? AJR Am J Roentgenol. 2002; 178(1):240. [ Özet ]
5) Huang X, Lee YZ, McKeown M, Gerig G, Gu H, Lin W, et al. Asymmetrical ventricular enlargement in Parkinson's disease. Movement Disorder. 2007; 22: 1657-1660. [ Özet ]
6) Jackler R, Brackmann DE. Neurotology, 2004, Mosby.1488p
7) Ng SE, Low AM, Tang KK et-al. Value of quantitative MRI biomarkers (Evans' index, aqueductal flow rate, and apparent diffusion coefficient) in idiopathic normal pressure hydrocephalus. J Magn Reson Imaging. 2009;30 (4): 708-15 [ Özet ]
8) The investigation of effects of vertigo, dizziness and imbalance on physical activity level, activities of daily living and quality of life in patient with peripheral vestibular hypofunction. 2016. www.acikarsiv.gazi.edu.tr/index.php?menu=2&secim=10&YayinBIK=14405 . Accessed September, 2016.
9) Camicioli R, Moore MM, Kinney A, Corbridge E, Glassberg K, Kaye JA. Parkinson's disease is associated with hippocampal atrophy. Mov Disord 2003; 18: 784-90. [ Özet ]
10) Breneis C, Seppi K, Schocke MF, Muller J, Luginger E, Bosch S, et al. Voxel-based morphometry detects cortical atrophy in the Parkinson variant of multiple system atrophy. Mov Disord 2003; 18:1132-8. [ Özet ]
11) Atasoy HT, Nuyan O, Tunc T, Yorubulut M, Unal AE, Inan LE. T2-weighted MRI in Parkinson's disease; substantia nigra pars compacta ypointensity correlates with the clinical scores. Neurol India. 2004; 52: 332-337. [ Özet ]
12) Geng DY, Li YX, Zee CS. Magnetic resonance imaging-based volumetric analysis of basal ganglia nuclei and substantia nigra in patients with Parkinson's disease. Neurosurgery. 2006; 58: 256-62. [ Özet ]
13) Schulz JB, Skalej M, Wedekind D, Luft AR, Abele M, Voigt K, et al. Magnetic resonance-imaging-based volumetry differentiates idiopathic Parkinson's syndrome from multiple system atrophy and progressive supranuclear palsy. Ann Neurol. 1999; 45: 65-74.
14) Harcherik DF, Cohen DJ, Ort S, Paul R, Shaywitz BA, Volkmar FR, Rothman SL, Leckman JF. Computed tomographic brain scanning in four neuropsychiatric disorders of childhood. Am J Psychiatry. 1985; 6: 731-734. [ Özet ]