


MRI FINDINGS IN SPONTANEOUS SPHENOID SINUS CEREBROSPINAL FLUID LEAKS
2Ankara Üniversitesi Tıp Fakültesi, Kulak Burun ve Boğaz Hastalıkları Ana Bilim Dalı, Ankara, Türkiye
Summary
Purpose:To evaluate patients with sphenoid sinus cerebrospinal fluid (CSF) leakage in terms of accompanying MRI findings suggestive of idiopathic intracranial hypertension (IIH).
Methods:
This retrospective study included 14 patients diagnosed with sphenoid sinus CSF leakage between 2012 and 2023. MRI examinations were performed using 1.5T or 3T scanners with T2-weighted fat suppressed, T2-weighted SPACE, and CISS images. Images were evaluated for empty sella, arachnoid pits, fluid in the optic nerve sheaths, vertical tortuosity of the optic nerves, Meckel's caves enlargement, sphenoid sinüs lateral recess pneumatization, and encephaloceles. Lateral recess pneumatization was defined as pneumatization extending beyond the line connecting the foramen rotundum and Vidian canal. Descriptive statistics were applied.
Results:
The mean age of the patients was 56 ± 12 years (13 females, 1 male). Arachnoid pits were observed in all patients, while empty sella and Meckel's cave enlargement were present in 86% and 79%, respectively. Encephaloceles were identified in 71% of cases, and lateral pneumatization was present in 64%. In 36% of patients, CSF leakage occurred without excessive sphenoid sinus pneumatization. Four patients had additional CSF leaks at the cribriform plate. Of the 12 patients who underwent CT prior to MRI, 10 showed a bony defect at the site of the leak.
Conclusion:
Sphenoid sinus CSF leaks are frequently associated with MRI findings such as empty sella, arachnoid pits, and Meckel's cave enlargement, which likely reflect underlying intracranial hypertension. Recognition of these features on MRI is crucial for accurate diagnosis, localization of the defect, and optimal surgical planning.
Introduction
Cerebrospinal fluid (CSF) leakage is a pathology that develops due to an osteodural defect between the subarachnoid space and the pneumatized structures of the skull base. Although CSF fistulas most commonly occur secondary to trauma, they may also develop spontaneously, although less frequently. The cribriform plate is the most common site of spontaneous CSF leakage. However, apart from the cribriform plate, leaks can occur anywhere along the skull base, with the sphenoid sinus and tegmen tympani being the other most frequently involved sites[1].CSF leaks of the sphenoid sinus may occur in the perisellar region or within the lateral recesses, the latter being the more common localization. Because of its close anatomical relationship with critical neurovascular structures, the management of sphenoid sinus CSF leaks can be more challenging. Visualization of leaks located in the lateral recesses is particularly difficult with a standard endonasal approach. In such cases, a transpterygoid approach is required to access and repair the defect. Therefore, preoperative localization of the leak site using imaging plays a crucial role in surgical planning[2].
It has been reported that sphenoid sinus CSF leaks may be associated with findings such as arachnoid pits, empty sella, and hyperpneumatization of the lateral recess[3]. The most likely mechanism for the development of CSF fistulas in the lateral recess of the sphenoid sinus is thought to be the coexistence of pneumatization of the lateral recess, localized bony flattening, and the presence of arachnoid pits in this region[1].
The aim of this study was to evaluate MRI findings of patients with CSF leakage, focusing on accompanying features detectable on CSF leak-dedicated sequences.
Methods
The institutional review board approved this single-center retrospective study. Patients with suspected CSF leakage who underwent MRI with a special protocol between 2012 and 2023 were evaluated. Images of 240 consecutive patients were assessed for CSF leakage by two neuroradiologist with 10 and 3 years of experience. Patients with leakage from sites other than the sphenoid sinus were excluded from the study (n = 220). Six out of 20 patients with a history of trauma or surgery of the sphenoid sinüs or cavernous sinus were also excluded. The remaining 14 patients with sphenoid sinüs CSF leakage formed the study group. Leakage was supported by surgical findings and beta-2 transferrin test. All imaging was performed using 3 Tesla (Verio, Siemens, Erlangen, Germany) or 1.5 Tesla (Aera, Siemens, Erlangen, Germany) MR scanners. The MRI protocol for CSF leakage consisted of T2 weighted fat suppressed coronal plane images with 3 mm slice thickness, T2-weighted sagittal plane SPACE images with 1 mm slice thickness, and CISS coronal plane images with 1 mm slice thickness. All images were evaluated by two radiologist with 4 years of experience in terms of empty sella, enlargement of the Meckel's caves (Figure 1), fluid in the optic nerve sheaths, vertical tortuosity of the optic nerves (Figure 2), arachnoid pits, encephaloceles (Figure 3), and lateral recess pneumatization of the sphenoid sinuses. Lateral recess pneumatization was defined as pneumatization lateral to the line connecting the foramen rotundum and the Vidian canal (Figure 4). The side of the leakage and the other accompanying sites of leakage were noted. The presence of a bony defect was evaluated on CT images (Figure 5).Descriptive statistics were used for data analysis. Continuous variables were presented as mean ± standard deviation [median (minimum?maximum)], and categorical variables were expressed as frequency and percentage.
 Büyütmek İçin Tıklayın |
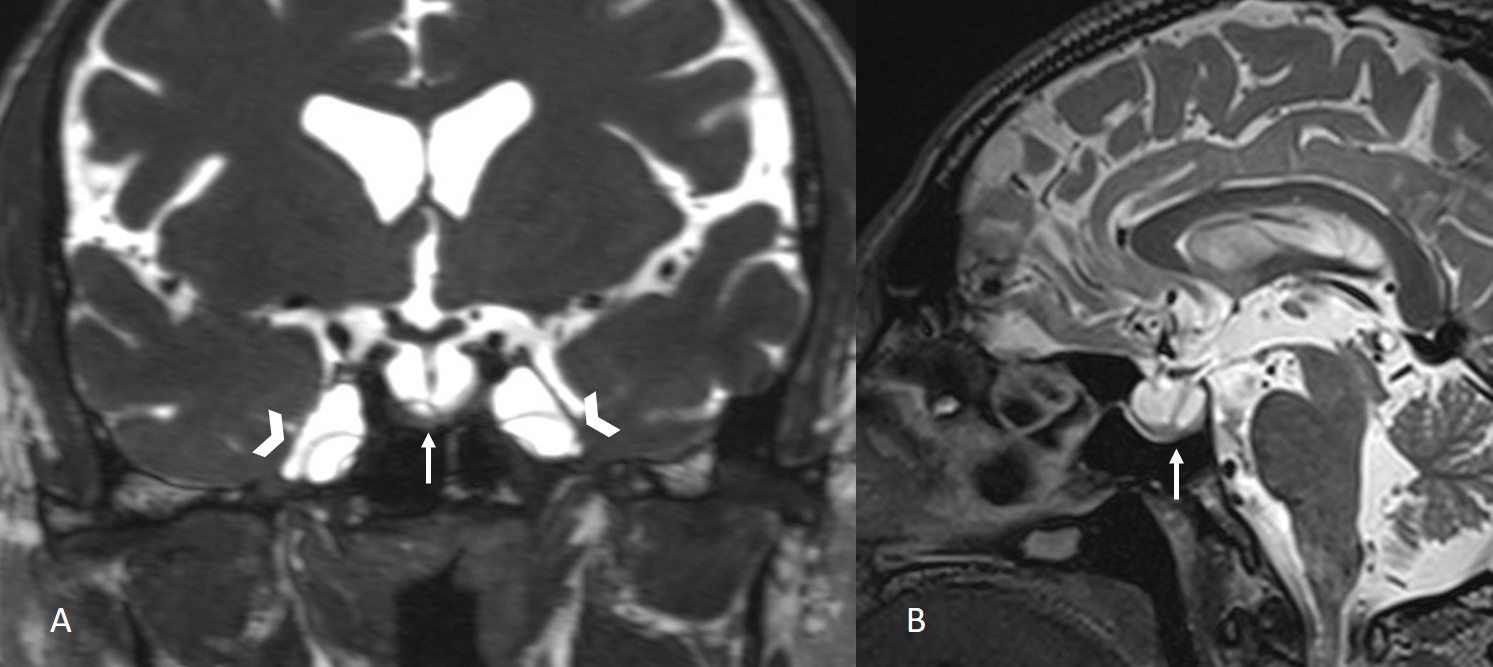
Figure 1: Coronal CISS image and sagittal T2-weighted SPACE image show empty sella (arrows) and enlargement of the Meckel's caves (arrowheads). |
 Büyütmek İçin Tıklayın |
Figure 2: Sagittal CISS images show fluid in the right (R) and the left (L) optic nerve sheaths (arrowheads) and tortuosity of the optic nerves (arrows). |
 Büyütmek İçin Tıklayın |
Figure 3: Axial T2-weighted SPACE image shows arachnoid pits (arrows) and encephalocele with CSF extending to the sphenoid sinus (arrowhead). |
 Büyütmek İçin Tıklayın |
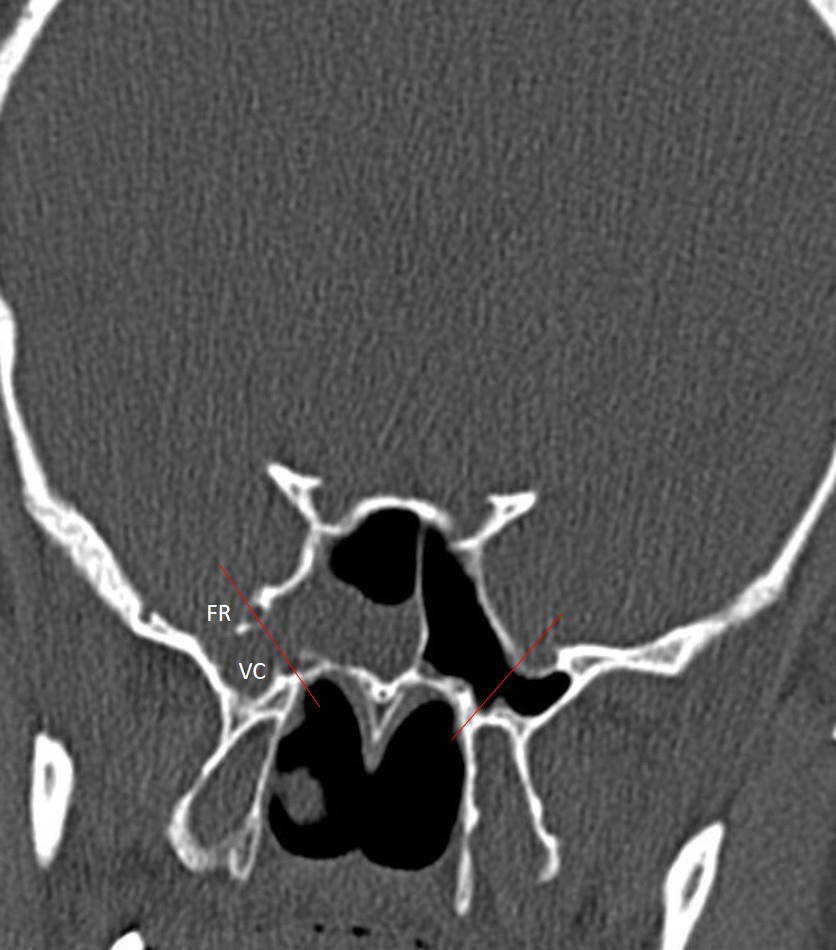
Figure 4: Coronal CT image of the sphenoid sinus showing the anatomical landmarks used to define lateral recess pneumatization. Lateral recess pneumatization was defined as pneumatization lateral to the line connecting the foramen rotundum (FR) and the Vidian canal (VC). |
 Büyütmek İçin Tıklayın |
Figure 5: Coronal CT image (A) shows bony defect (arrow) in the left sphenoid sinus lateral wall and coronal CISS image (B) show CSF (arrowhead) in the left sphenoid sinus. |
Results
The mean age of patients was 56±12 years (13 females and 1 male).Among the study group, arachnoid pits were observed in all patients, while encephalocele was identified in 10 patients (71%). Empty sella was the second most common finding and observed in 12 patients (86%). Increased fluid in the optic nerve sheaths and vertical tortuosity of the optic nerves were noted in 9 patients (both 64%). Enlargement of Meckel's caves was present in 11 patients (79%). Lateral pneumatization of the sphenoid sinuses was seen in 9 patients (64%). In 36% of the cases, CSF leakage was present without excessive pneumatization of the sphenoid sinus. In 4 patients, in addition to the CSF leak observed in the sphenoid sinus, an additional leak was also detected at the level of the cribriform plate.
Evaluation of CSF leaks according to their location within the sphenoid sinus revealed that 5 (36%) were on the right side, 4 (29%) on the left side, 2 (14%) were bilateral, 1 (7%) was located anteriorly, and 2 (14%) posteriorly.
Twelve patients had undergone CT before MRI, and in 10 of these cases, a bony defect was identified on CT at the site of the CSF leak.
Discussion
In this retrospective study, MRI findings of 14 patients with sphenoid sinus CSF leaks were evaluated. The most common accompanying imaging features were empty sella, Meckel's cave enlargement, and arachnoid pits, which are frequently described in association with spontaneous CSF leaks and idiopathic intracranial hypertension (IIH). These findings are consistent with previous studies reporting that radiologic markers of chronically increased intracranial pressure, such as empty sella and arachnoid pits, are often present in patients with spontaneous skull base CSF leaks[3,4].Previous studies have suggested that spontaneous CSF leaks of the sphenoid sinus are most often related to defects in the lateral recess[3,5]. In our study, 64% of patients had lateral pneumatization of the sphenoid sinus, and the majority of leaks were located in the lateral recess. This aligns with the observations of Shetty et al.[3], who found that extensive pneumatization of the lateral recess predisposes the thin bony walls to erosion and subsequent CSF leakage. The absence of excessive pneumatization in 36% of our patients, however, can indicate that other anatomic or physiologic factors, such as bone remodeling due to sustained intracranial pressure, may also contribute to defect formation.
The coexistence of arachnoid pits, Meckel's cave enlargement, and empty sella in most of our cases supports the hypothesis that chronically elevated intracranial pressure plays a key role in the pathogenesis of spontaneous sphenoid sinus CSF leaks. Repetitive CSF pulsations through arachnoid pits can result in bone thinning and herniation of meninges or brain tissue, leading to encephalocele formation and osteodural defects[1].
From a clinical perspective, the identification of imaging findings such as lateral pneumatization, arachnoid pits, and encephaloceles has important implications for surgical planning. Visualization of defects in the lateral recess is challenging with a standard endonasal approach, and a transpterygoid route may be required for adequate exposure[2]. Accurate preoperative localization of the defect on MRI is therefore essential to ensure a successful repair and to minimize the risk of recurrence.
This study has certain limitations, primarily its small sample size and retrospective design, which restrict statistical analysis and generalizability. Additionally, it was not known whether the patients had a clinically established diagnosis of IIH and the evaluation was based solely on the indirect imaging findings of IIH. Nevertheless, our results contribute to the evidence suggesting that anatomical variations of the sphenoid sinus and radiologic markers of increased intracranial pressure are key factors in the development of spontaneous CSF leaks.
In conclusion, sphenoid sinus CSF leaks are frequently associated with imaging features such as empty sella, arachnoid pits, and Meckel's cave enlargement, which likely reflect underlying intracranial hypertension. Recognition of these findings on dedicated MRI sequences is essential for accurate diagnosis, determination of the defect location, and appropriate surgical planning.
Reference
1) Alonso RC, de la Peña MJ, Caicoya AG, Rodriguez MR, Moreno EA, de Vega Fernandez VM. Spontaneous skull base meningoencephaloceles and cerebrospinal fluid fistulas. Radiographics. 2013 Mar-Apr;33(2):553-70. doi: 10.1148/rg.332125028. [ Özet ]
2) Shah K, Konar S, Shukla D, Sadashiva N, Srinivas D, Arimappamagan A, Prabhuraj AR. Management of cerebrospinal fluid leaks from lateral sphenoid sinus wall: Tailored approach based on proposed zone-wise classification. J Clin Neurosci. 2025 Jul;137:111331. doi: 10.1016/j.jocn.2025.111331. [ Özet ]
3) Shetty PG, Shroff MM, Fatterpekar GM, Sahani DV, Kirtane MV. A retrospective analysis of spontaneous sphenoid sinus fistula: MR and CT findings. AJNR Am J Neuroradiol. 2000 Feb;21(2):337-42. [ Özet ]
4) Schuknecht B, Simmen D, Briner HR, Holzmann D. Nontraumatic skull base defects with spontaneous CSF rhinorrhea and arachnoid herniation: imaging findings and correlation with endoscopic sinus surgery in 27 patients. AJNR Am J Neuroradiol. 2008 Mar;29(3):542-9. doi: 10.3174/ajnr.A0840. [ Özet ]
5) Woodworth BA, Prince A, Chiu AG, Cohen NA, Schlosser RJ, Bolger WE, Kennedy DW, Palmer JN. Spontaneous CSF leaks: a paradigm for definitive repair and management of intracranial hypertension. Otolaryngol Head Neck Surg. 2008 Jun;138(6):715-20. doi: 10.1016/j.otohns.2008.02.010. [ Özet ]