


AGE EFFECT ON TYMPANOMETRIC EVALUATION RESULTS
2Nişantaşı Üniversitesi, Odyometri, İstanbul, Turkey
3Bingöl Üniversitesi, Odyometri, Bingol, Turkey
4İstanbul Prof. Dr. Cemil Taşcıoğlu Şehir Hastanesi, Odyoloji, İstanbul, Turkey
5Marmara Üniversitesi, Odyoloji, İstanbul, Turkey
Summary
Introduction: With increasing age, changes occur in the anatomy and physiology of the outer and middle ear, which are reflected in the tympanometric results. This study aimed to evaluate the effect of age on tympanometric evaluation results in participants.Material and Methods: Tympanometric evaluation results were obtained with Titan® wideband tympanometry from 46 individuals between the ages of 6-18, 52 individuals between the ages of 19-39, and 37 individuals between the ages of 40-60 with normal hearing, normal otoscopic findings, and type A tympanogram were examined retrospectively. A total of 265 ears were evaluated, and comparison and regression analysis were performed according to age groups to determine the effect of age on compliance, tympanometric peak pressure, tympanometric width, equivalent ear canal volume, and resonance frequency.
Results: The statistical evaluation revealed that age affected compliance, tympanometric peak pressure, tympanometric width, equivalent ear canal volume, and resonance frequency. No significant difference was observed between the tympanometric results of the right and left ears.
Conclusion: It is known that tympanometric evaluation results vary in terms of age, gender, and ethnic characteristics. This study revealed the effects of age on tympanometric evaluation results. These differences were thought to be due to differences in body size between adults and children and changes in middle ear physiology and anatomy with age. Our study is believed to contribute to the literature by revealing age-related changes in tympanometric results.
Introduction
The outer and middle ear structures change with development and reach adult form of around the age of nine[1]. However, changes in these structures continue throughout life. Changes in the outer and middle ear associated with aging have been documented in the literature[2]. These include a collapse of the cartilaginous external ear canal, increased stiffness in the tympanic membrane and ossicular chain, decrease in epithelial cell production, aging of extracellular substances (elastic tissue, cartilage, and bone), and extracellular accumulation of various substances[3-5]. It has also been stated that aging may lead to degeneration of the outer and middle ear with structural changes in the tissue epithelium, ceruminal gland atrophy, degeneration of the incudomalleal and incudostapedial joints, and tensor tympani and stapedius muscle atrophy. These changes can reduce the efficiency of sound transmission to the middle ear, thus causing decreased hearing sensitivity[2].Tympanometry is defined as a sensitive, specific, non-invasive, simple technique that measures acoustic impedance or admittance as a function of pressure in the ear canal to analyze the acoustic properties of the middle ear system[6,7]. With multifrequency tympanometry, in addition to the parameters evaluated with conventional tympanometry [compliance (Ya), equivalent ear canal volume (ECV), tympanometric peak pressure (TPP), and tympanometric width (TW)], resonance frequency (RF) measurement can also be performed. RF, which reflects the frequency value where mass and stiffness effects are equal in magnitude, is the frequency value where the sum of mass and stiffness effects is "0". The middle ear transmits a sound at a frequency equal to the RF more easily than other frequencies[6]. The RF shifts towards lower frequencies as the mass in the middle ear increases and towards higher frequencies as the stiffness increases[8].
Studies have shown that tympanometric measurements in healthy individuals may differ depending on age, gender, and ethnic characteristics. In addition, it is important to determine normative data and their standards to distinguish normal and pathological conditions correctly[2] When the literature was reviewed, although normative values of tympanometric results were found in different age groups, there were not enough studies comparing tympanometric results of different age groups. Our study aims to evaluate the possible effects of age on tympanometric results.
Methods
This retrospective study was conducted using the tympanometric results of patients with different age groups who applied to Bezmialem Vakıf University Audiology Clinic between 01.01.2018 and 01.01.2023 and whose otological examination was normal. The study was approved by the Bezmialem Vakıf University Non-Interventional Research Ethics Committee with decision number 2023/240 on 26.07.2023, and it was conducted in accordance with the ethical principles specified in the Declaration of Helsinki. Individuals with normal pure tone average and normal middle ear function were included in the study.In the retrospective audiometric evaluation, air conduction thresholds at octave frequencies between 250-8000 Hz and bone conduction thresholds at frequencies between 250-4000 Hz were examined in pure tone audiometry. Tympanometric results of participants whose air-bone gap between 250-4000 Hz was <10 dB HL and air conduction threshold between 250-8000 Hz was 15 dB HL or better were examined.
The conventional tympanometry and RF were evaluated with the Titan® tympanometry (Interacoustics, Denmark) featuring wideband tympanometry and analyzed retrospectively. RF measurements were made using a narrow band click stimulus with a frequency range of 226 Hz - 8000 Hz, a duration of 2 msec, a rate of 21.5/sec, and an intensity level of 100 dB peSPL (≈65 dB nHL). 226 Hz probe tone at 85 dB SPL was used for conventional tympanometry, and the pressure ranged from (+200) to (-400) to measure compliance at tympanometric peak pressure. After the probe was appropriately placed in the patient's external ear canal, measurements were recorded via Titan Suite software (Interacoustics, Denmark).
Participants
Ears that met the inclusion criteria and had normal otoscopic findings and type A tympanogram were evaluated. Participants were divided into different age groups between 6-18 years, 19-39 years, and 40-60 years, and tympanometric evaluation results were compared according to age. Data obtained from 46 individuals (90 ears) between the ages of 6-18, 52 individuals (102 ears) between the ages of 19-39, and 37 individuals (73 ears) between the ages of 40-60 were included in the study. The average age (mean ± SD) in the 6-18, 19-39, and 40-60 age groups are 10.5 ± 2.96; 24.58 ± 5.03; 47.81 ± 6.42 respectively.
The resonance frequency, equivalent ear canal volume, tympanometric peak pressure, compliance, and tympanometric width were analyzed and compared according to age. The data of individuals who were evaluated using the Interacoustics Titan device between 01.01.2018 and 01.01.2023 and met the inclusion criteria were withdrawn from the software.
Statistical analysis
All statistical analyses were analyzed and reported in the IBM SPSS Statistics 22.0 program and at a 95% confidence level. Considering previous studies, the sample size was determined to be at least 100 to obtain 80% power at a 95% confidence level. Results were analyzed and reported at the α=0.05 significance level. The distribution of the data was examined using the Shapiro-Wilk test. Independent Samples t-test was used in groups showing normal distribution compared to right and left ears; Mann Whitney U test was used in groups that did not show normal distribution. In comparing data between different age groups, the One-Way Anova test and posthoc Tamhane test were used in groups with normal distribution, while the Kruskal Wallis test and posthoc Bonferroni correction test were used in groups with non-normal distribution. Descriptive statistics of the data are given as mean ± S. Deviation and min-max. Also, regression analysis was performed to determine the effect of age on tympanometric values.
Results
In this study, tympanometric evaluation results of 46 individuals (90 ears) aged 6-18 years (mean ± SD; 10.5 ± 2.96), 52 individuals (102 ears) aged 19-39 years (mean ± SD; 24.58 ± 5.03), and 37 individuals (73 ears) aged 40-60 years (mean ± SD; 47.81 ± 6.42) were included. Ear-specific comparisons, age group comparisons, and regression analysis of tympanometric findings were analyzed.As a result of pairwise comparison of the right and left ears, no ear-specific differences were observed in tympanometric evaluation results (Table 1). Since the ear effect was not significant, the age effect was not evaluated on ear based.
){kind=link}
Table 1: Comparison of tympanometric results in right and left ears in different age groups
Kruskal Wallis Test and post hoc Bonferroni correction for pairwise comparisons were performed for statistical evaluation of Ya, TPP, TW, and ECV findings. Significant differences between different age groups were observed in all tympanometric findings, as shown in Table 2.
){kind=link}
Table 2: Tympanometric results of different age groups
As a result of the statistical evaluation, Ya was significantly lower in the 19-39 age group than in the 40-60 and 6-18 age groups. TPP is significantly lower in the 6-18 age group than in the 19-39 age group. TW was significantly lower in the 40-60 age group than in the 6-18 and 19-39 age groups. The ECV is significantly greater in the 40-60 age group than in the 6-18 and 19-39 age groups and is significantly greater in the 19-39 age group than in the 6-18 age group.
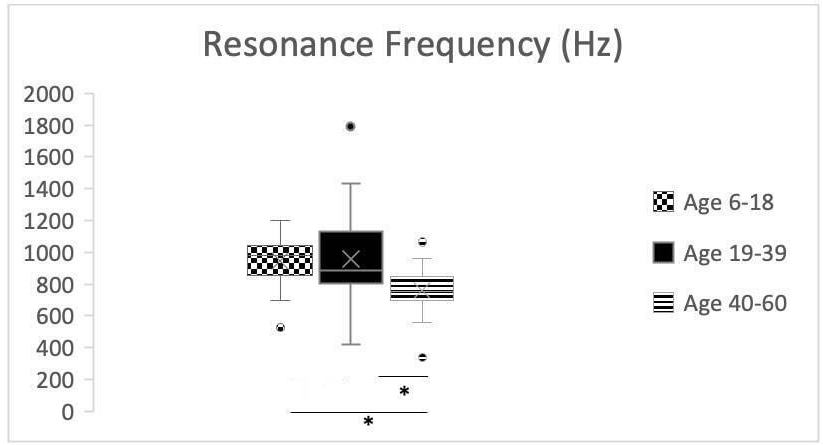
ANOVA and post hoc Tamhane test results showed that the resonance frequency was significantly lower in the 40-60 age group compared to the 6-18 and 19-39 age groups (Figure 1).
 Büyütmek İçin Tıklayın |
Figure 1: Resonance frequency comparison by age (*p<0.05) |
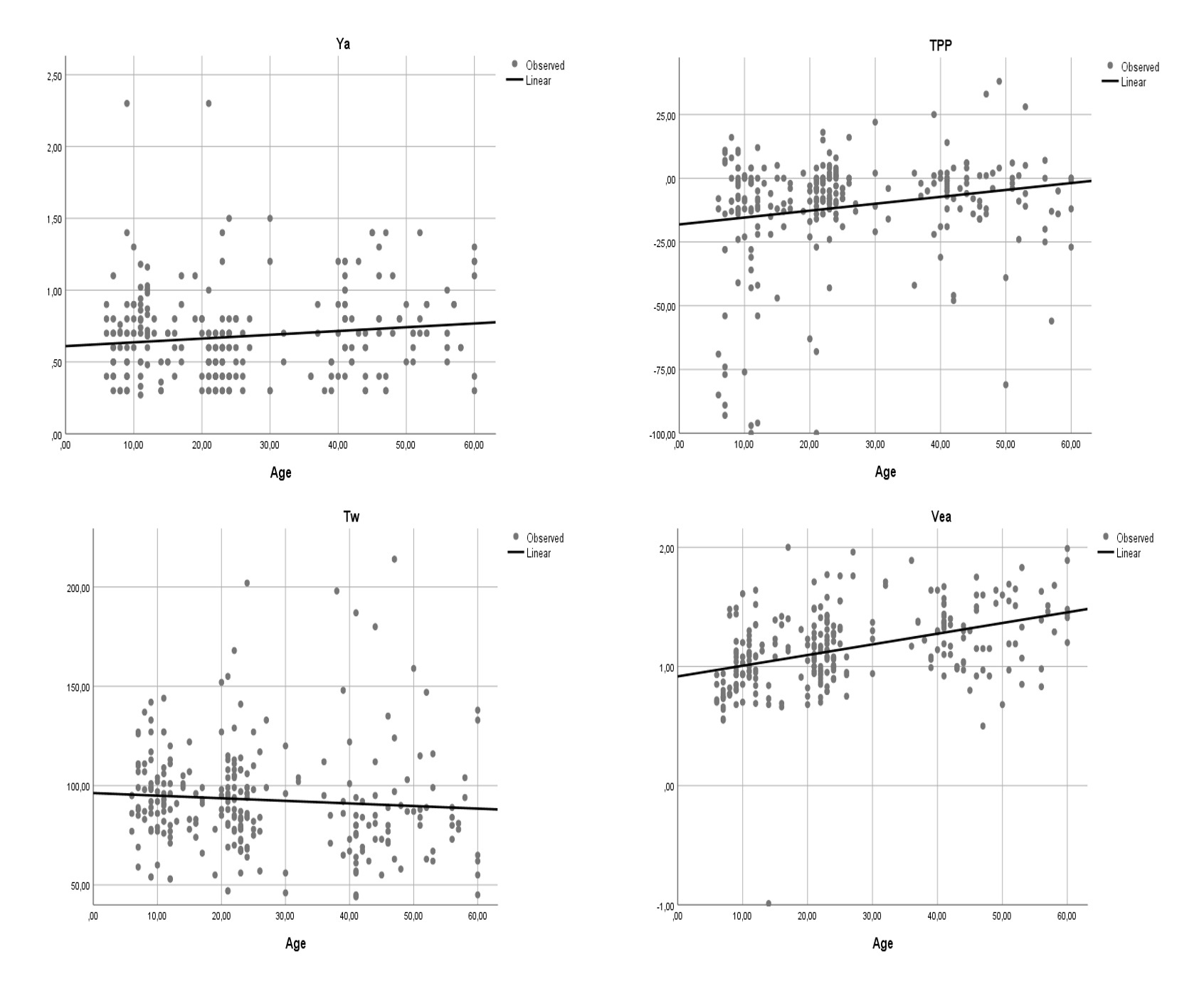
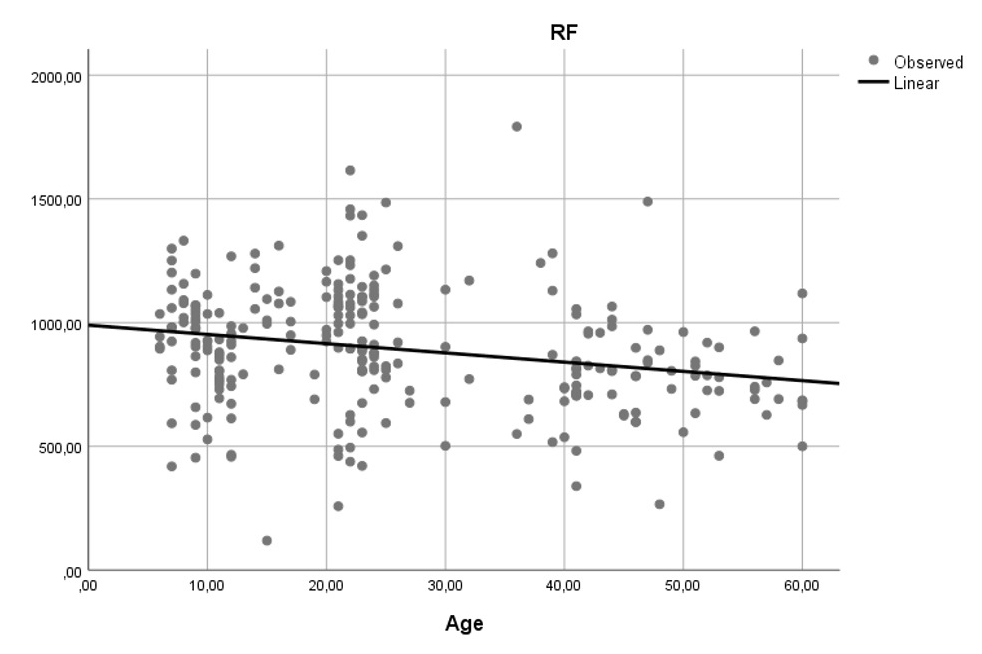
The regression analysis determined that Ya, ECV, and TPP values increased statistically significantly with age (Figure 2), while RF values decreased significantly with increasing age (Figure 3). No significant change was observed in TW according to age. The regression analysis results are detailed in Table 3.
){kind=link}
 Büyütmek İçin Tıklayın |
Figure 2: Regression analysis of the aging effect on tympanometric results |
 Büyütmek İçin Tıklayın |
Figure 3: Regression analysis of resonance frequency |
Table 3: Regression analysis of the aging effect on tympanometric results
Discussion
Tympanometry is a technique that measures acoustic impedance or admittance as a function of pressure in the ear canal to analyze the acoustic properties of the middle ear system[6]. Tympanometry, a routine part of audiological/otological evaluation, is a safe and rapid gold standard method to evaluate middle ear function[9,10]. In addition to Ya, TPP, ECV, and TW are measured in traditional tympanometry, and RF can also be measured in multifrequency tympanometry and wideband tympanometry. Studies have shown that body size, age, and ethnicity can affect resonance frequency and other tympanometric findings[11]. Our study aimed to show the age-related effects of Ya, TPP, ECV, TW, and RF in participants of different age groups.When the literature was reviewed, no study observed differences in tympanometric findings between the right and left ears[10,12,13]. In our study, no significant difference was found between the right and left ears of the participants, supporting the literature (p>0.05). This finding is consistent with the absence of a significant anatomical and physiological difference in the right and left middle ear.
Since studies have shown that ethnicity affects tympanometric results, comparing the age effect in groups of the same ethnicity will provide more accurate results[10,14]. In this regard, when studies evaluating tympanometric findings in Turkish participants were examined, there were not enough studies that evaluated age-related effects on tympanometric findings in participants with normal middle ear function in similar age groups. Changes observed in the middle and outer ear structures depending on age and ethnicity point to a deficiency in the literature on this subject.
Looking at the anatomical changes that occur with aging, arthritis in the ossicular joints or a stiffer tympanic membrane causes increased stiffness. In comparison, a thicker tympanic membrane and accumulation of calcium molecules cause an increase in mass. These degenerative changes affect individuals to varying degrees[15]. Studies agree that age affects tympanometric results[16-18]. With age, the tympanic membrane becomes stiffened, thinner, and less vascular; calcification in the malleus, incus, and stapes joints, ossification and calcification in the eustachian tube, and atrophy and degeneration in the middle ear muscles can be observed[19]. Although our study had significant differences in ECV, Ya, TW, TPP, and RF with age and these findings support the literature.
The RF is affected by mass and/or stiffness changes in the mechano-acoustic system of the middle ear. While RF increases in pathologies that increase the system's stiffness, such as otosclerosis and rheumatoid arthritis, RF decreases in pathologies where middle ear stiffness decreases, such as ossicular chain disruption and otitis media with effusion. The normal range of RF values reported for adults with normal hearing varies, but most studies suggest that the RF range for the middle ear is between 800 and 1200 Hz[9,10]. Kaya et al., evaluated resonance frequency in 60 healthy adults aged 19-45. The findings obtained in their study are similar to the data for the 19-39 age group in our study. In their study, regardless of gender difference, the middle ear resonance frequency was found to be 900 Hz on average in Turkish participants, while in our study, the average resonance frequency in the 19-39 age group was similarly obtained as 955 Hz[12]. In the literature, it has been reported that the average middle ear resonance frequency is 1003 Hz in children aged 6-15, while it is 817 Hz for individuals aged 20-40[20,21]. These differences can be attributed to the difference in body size between adults and children. Larger ear sizes in adults will cause the middle ear volume to be larger, so middle ear systems will have lower resonance frequencies[21]. Similarly, in our study, the RF was significantly lower in the 40-60 age group.
ECV varies according to both gender and age. ECV is smaller in women than men at all ages, with an average difference of 0.2 cm3 in adulthood. Given the wide range of normal values, it has been reported that separate norms are not required for men and women, but different norms are needed for children and adults. ECV has been observed to increase from an average of 0.6 cm3 in children younger than seven years to 0.8 cm3 between 6 and 15 years of age and 1.4 cm3 in adulthood[16-18]. In our study, ECV value increased significantly with age. Average ECV values were obtained as 0.99 ml, 1.18 ml, and 1.31 ml in the 6-18, 19-39, 40-60 age groups, respectively.
Ya evaluates the elastic properties of the tympanic membrane in tympanometry. Therefore, tympanometry has been used to investigate age-related changes in compliance, but there is no consensus on this issue in the literature. Beattie and Leamy reported a significantly increased admittance with age when they compared the group consisting of participants with an average age of 65 with normal audiometric and otoscopic findings and the group with an average age of 20[22]. Creten et al. found no change in susceptance and conductance values among eight different groups of different ages, while Gates et al. reported in their study on a large population that compliance decreased significantly with increasing age[23,24]. In their study investigating the age-related absorbance change, Şahin and Aksoy did not find any significant age-related difference in the absorbance in participants with normal middle ear function between the ages of 20-29, 30-39, and 40-49, and they found that the absorbance did not change between the ages of 20-49. As stated by Şahin and Aksoy in their study, the small age difference between the groups may not have caused a difference in the middle ear system that would cause a change in absorbance[25]. In our study, tympanometry was evaluated in broader age ranges, and it was found that Ya decreased significantly in the 19-39 age group compared to the 6-18 and 40-60 age groups. More studies are needed on this subject to understand the effect of age on compliance.
TW measures the sharpness of the tympanogram. The presence of a middle ear infection reduces the slope and increases the width of the tympanogram[26]. Apart from this, age can also affect TW, young adults aged 20-30 years have a narrower TW than children[27], and older adults aged 48-90 years have a narrower TW than young adults[17]. However, in the literature, some studies find a significant difference in TW with age[7,17,27], and some do not observe a significant change with age[13,28]. In our study, a significant decrease in TW was observed between the ages of 40-60, but no significant change in TW was observed with age in the regression analysis.
Conclusion
In our study, the effect of age on tympanometric findings was shown. These differences are attributed to differences in body size between adults and children and changes in middle ear physiology with age. It is important to establish norms for a specific measurement using a specific tool in a specific population and to determine normal and pathological conditions accordingly. In this context, it is thought that our study will contribute to the literature by presenting the tympanometric evaluation results for the relevant age groups of Turkish participants with normal middle ear function and revealing the effect of age on tympanometric findings.Reference
1) Calandruccio L, Fitzgerald TS, Prieve BA. Normative multifrequency tympanometry in infants and toddlers. J Am Acad Audiol. 2006;17(07):470-80. [ Özet ]
2) Mazlan R, Kei J, Ya CL, Yusof WNHM, Saim L, Zhao F. Age and gender effects on wideband absorbance in adults with normal outer and middle ear function. Journal of Speech, Language, and Hearing Research. 2015;58(4):1377-86. [ Özet ]
3) Randolph LJ, Schow RL. Threshold inaccuracies in an elderly clinical population: ear canal collapse as a possible cause. Journal of Speech, Language, and Hearing Research. 1983;26(1):54-8. [ Özet ]
4) Ruah CB, Schachern PA, Zelterman D, Paparella MM, Yoon TH. Age-related morphologic changes in the human tympanic membrane: a light and electron microscopic study. Arch Otolaryngol Head Neck Surg. 1991;117(6):627-34. [ Özet ]
5) Hinojosa R, Naunton RF. Presbycusis. Otolaryngology. 1980;2:1777-87.
6) Colletti V. Multifrequency tympanometry. Audiology. 1977;16(4):278-87. [ Özet ]
7) Holte L. Aging effects in multifrequency tympanometry. Ear Hear. 1996;17(1):12-8. [ Özet ]
8) Shanks J, Shelton C. Basic principles and clinical applications of tympanometry. Otolaryngol Clin North Am. 1991;24(2):299-328. [ Özet ]
9) Margolis RH, Goycoolea HG. Multifrequency tympanometry in normal adults. Ear Hear. 1993;14(6):408-13. [ Özet ]
10) Shahnaz N, Davies D. Standard and multifrequency tympanometric norms for Caucasian and Chinese young adults. Ear Hear. 2006;27(1):75-90. [ Özet ]
11) Iacovou E, Vlastarakos P V, Ferekidis E, Nikolopoulos TP. Multi-frequency tympanometry: clinical applications for the assessment of the middle ear status. Indian Journal of Otolaryngology and Head & Neck Surgery. 2013;65:283-7. [ Özet ]
12) Kaya Ş, Karabulut M, Keseroğlu K, Dağlı M, Korkmaz MH, Er S. Sağlıklı Yetişkinlerde Multi-Frekans Timpanometri ve Orta Kulak Rezonans Frekansı: Klinik Normatif Değerler. KBB-Forum. 2020;19(1):27-33. [ 13) Manchaiah V, Durisala N, Marimuthu V. Tympanometric profiles for Chinese older adults. Audiol Res. 2017;7(2):190. [ Özet ]
14) Wan IKK, Wong LLN. Tympanometric norms for Chinese young adults. Ear Hear. 2002;23(5):416-21. [ Özet ]
15) Uchida Y, Nomura H, Itoh A, Nakashima T, Ando F, Niino N, et al. The effects of age on hearing and middle ear function. J Epidemiol. 2000;10(1sup):26-32. [ Özet ]
16) Shanks JE, Stelmachowicz PG, Beauchaine KL, Schulte L. Equivalent ear canal volumes in children pre-and post-tympanostomy tube insertion. Journal of Speech, Language, and Hearing Research. 1992;35(4):936-41. [ Özet ]
17) Wiley TL, Cruickshanks KJ, Nondahl DM, Tweed TS, Klein R, Klein BE. Tympanometric measures in older adults. J Am Acad Audiol. 1996;7(4):260-8. [ Özet ]
18) Haapaniemi JJ. Immittance findings in school-aged children. Ear Hear. 1996;17(1):19-27. [ Özet ]
19) Özdemir D, Mehel DM, Çeçen AB, Özdemir Ş, Küçüköner Ö, Özgür A. Evaluation of age-related changes in middle-ear structures by wideband tympanometry. Acta Otolaryngol. 2022;142(6):505-8. [ Özet ]
20) Hanks WD, Rose KJ. Middle ear resonance and acoustic immittance measures in children. Journal of Speech, Language, and Hearing Research. 1993;36(1):218-22. [ Özet ]
21) Shahnaz N, Feeney MP, Schairer KS. Wideband acoustic immittance normative data: ethnicity, gender, aging, and instrumentation. Ear Hear. 2013;34:27s-35s. [ Özet ]
22) Beattıe RC, Leamy DP. Otoadmittance: Normative values, procedural variables, and reliability. Ear Hear. 1975;1(1):21-7.
23) Gates GA, Cooper Jr JC, Kannel WB, Miller NJ. Hearing in the elderly: The Framingham Cohort, 1983-1985: Part 1. Basic audiometric test results. Ear Hear. 1990;11(4):247-56. [ Özet ]
24) Creten WL, Van de Heyning PH, Van Camp KJ. Immittance Audiometry Normative Data at 220 and 660 Hz. Scand Audiol. 1985;14(3):115-21. [ Özet ]
25) Şahin M, Aksoy S. Examination of Wideband Tympanometry (WBT) Parameters in Individuals with Healthy Middle Ear. Hacettepe University Faculty of Health Sciences Journal. 2021;8(1):77-90.
26) Katz J, Chasin M, English KM, Hood LJ, Tillery KL. Handbook of clinical audiology. Vol. 7. Wolters Kluwer Health Philadelphia, PA; 2015.
27) Roup CM, Wiley TL, Safady SH, Stoppenbach DT. Tympanometric screening norms for adults. 1998;7(2):55-60. [ Özet ]
![]() Tam Metin ]
Tam Metin ]