


BILATERAL RANULA IN AN ELDERLY PATIENT: A CASE REPORT
2Selçuk University Meram Faculty of Medicine, Department of Patology, Konya, Turkey
Summary
Ranula is a mucus extravasation cyst arising from the sublingual gland. Ranula usually appears as a painless, fluctuant swelling. It commonly occurs unilaterally and in young adults. Bilateral ranula is extremely rare. A 53 year-old female suffered from bilateral swelling in the floor of the mouth that had been enlarging slowly over the past 6 months. The lesions were resected completely via intraoral approach. No complication was observed during the postoperative period. There was no recurrence in the seven months follow up period.Introduction
Ranula is a retention cyst arising from the sublingual gland on the floor of the mouth as a result of ductal obstruction and fluid retention. Ranulas can be divided into three types; sublingual, plunging, and sublingual-plunging. A sublingual ranula develops in the floor of the mouth, while a plunging ranula is recognized as a soft cystic swelling in the submandibular or upper cervical region. When a sublingual ranula has a cervical extension through the mylohyoid muscle, the term “sublingual-plunging ranula” is used [1].Ranula may be seen at birth or in later life [2]. It is commonly seen in young adult. Ranula commonly occurs unilaterally, and bilateral ranulas are extremely rare [2-4]. There has no report about simultaneous bilateral ranula occurring in an elderly patient in the English language literature until now.
Case Presentation
A 53-year-old woman suffered from painless, cystic masses, which located on the floor of the mouth bilaterally (Fig 1). They had been enlarging progressively over the past 6 months. Physical examination revealed tense, fluctuant, bluish, cystic lesions that measured 1x1 cm in the right and 2x2 cm in the left sublingual area. The tongue was painful and displaced on the upper side of the mouth. There was no history of local trauma or surgery. Patient’s medical and family histories were also unremarkable. Under general anesthesia, the cyst was removed with sublingual gland on the left side and by extracapsulary dissection on the right side using an intraoral approach. Histopathologic evaluations of both lesions were performed (Fig. 2). There was no complication during the postoperative period. At the seven months after surgery, there was no recurrence.
 Büyütmek İçin Tıklayın |
Figure 1: Intraoral view of the bilateral ranula |
 Büyütmek İçin Tıklayın |
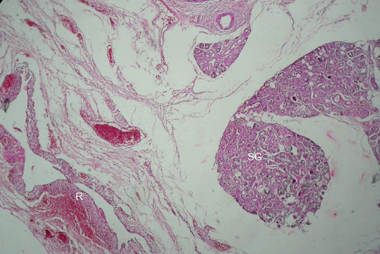
Figure 2: Microscopic examination shows the absence of epithelial tissue in the pseudocyst wall (H&E x4) (R: Ranula, SG: Salivary gland) |
Discussion
Most of the patients with oral ranula presented with a gradually enlarging swelling of the floor the mouth. The lesion is painless, fluctuant and round or oval. It may drain spontaneously at intervals [5]. The etiology of ranula is unknown; however, obstruction, trauma, and congenital anomalies have been implicated [6-9]. The diagnosis of ranula is generally based on the clinical examination and sometimes on computerized tomography or magnetic resonance imaging findings for the plunging lesion. A fine-needle aspiration biopsy may be helpful in demonstrating the mucus with inflammatory cells. Chemical analysis of aspiration fluid can reveal high amylase and protein contents. Sialography provides minimal information in this lesion [6,7,9].The differential diagnosis of ranula should include masses and swellings in the floor of the mouth and submandibular space region. These are dermoid and epidermoid cysts, branchial cleft cysts, thyroglossal duct cysts, cystic hygroma, lipomas, abscess, and malignant neoplasia [6,7,10]. Histologically, ranula consists of a central cystic space containing mucin and a pseudocyst wall composed of loose, vascularized connective tissues. Histiocytes predominate in the pseudocyst wall, but over time, these become less prominent. An important feature in the histologic diagnosis is the absence of epithelial tissues in the pseudocyst wall [8,11].
A variety of procedures have been proposed for ranula, including incision and drainage, marsupialization, irradiation, injection of sclerosing agents, cyst extirpation, and excision of the sublingual gland with the lesion [5,7,10,12]. The incision and drainage, and marsupialization have high recurrence rates. Crysdale et al [13] reported that the recurrence rate was 100% in cases with incision and drainage, 61% in cases of simple marsupialization, and 0% in cases of excision of the ranula with or without sublingual gland excision. Zhao et al [5] reported that the recurrence rates for marsupialization, excision of ranula, and excision of the sublingual gland or excision of the gland combinated with lesion were 66.67%, 57.69%, and 1.20%, respectively. The excision of the sublingual gland or ranula may carry the potential risk of the severe hemorrhage from the sublingual vasculature, lingual nerve damage, and duct injuries. Choi and Oh [14] used hydrodissection technique in the treatment of ranulas and they noted less bleeding, fewer incidents of neural and sort tissue damage, and a lower recurrence rate. This procedure involves the injection under pressure of saline and lidocaine with 1: 100,000 of epinephrine into the dissection plane [14].
In conclusion, bilateral ranulas are extremely rare. The incision and drainage, and marsupialization have high recurrence rates. Excision of ranula or excision of the sublingual gland combinated with lesion is suitable and effective method for intraoral ranulas.
Reference
1) Horiguchi H, Kakuta S, Nagumo M. Bilateral plunging ranula. A case report. Int J Oral Maxillofac Surg. 1995 ; 24:174-5. [ Özet ]
2) Barker GR. Bilateral ranula. Int J Oral Surg. 1984; 13:352-4. [ Özet ]
3) Kinirons MJ. Bilateral ranulae in a neonate: a case report. J Oral Med. 1983; 38:56-7. [ Özet ]
4) Saheeb BD. Recurrent congenital bilateral ranula: a case report. SADJ. 2001; 56:366-8. (Abstract). [ Özet ]
5) Zhao YF, Jia Y, Chen XM, Zhang WF. Clinical review of 580 ranulas. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004; 98:281-7. [ Özet ]
6) Parekh D, Stewart M, Joseph C, Lawson HH. Plunging ranula: a report of 3 cases and review of the literature. Br J Surg 1987; 74:307-9. [ Özet ]
7) Anastassov GE, Haiavy J, Solodnik P, Lee H, Lumerman H. Submandibular gland mucocele: diagnosis and management. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000; 89:59-63. [ Özet ]
8) Davison MJ, Morton RP, McIvor NP. Plunging ranula: clinical observations. Head Neck 1998; 20:63-8. [ Özet ]
9) Özcan C., Ünal M., Görür K. Servikal (Plunging) Ranula: Olgu Sunumu. Turk Arch Otolaryngol 2001; 39: 47-50.
10) Yuca K, Bayram I, Cankaya H, Caksen H, Kiroglu AF, Kiris M. Pediatric intraoral ranulas: an analysis of nine cases. Tohoku J Exp Med. 2005; 205:151-5. [ Özet ]
11) Batsakis JG, McClatchey KD. Cervical ranulas. An Otol Rhinol Laryngol 1988; 97:561-2. [ Özet ]
12) Zhao YF, Jia J, Jia Y. Complications associated with surgical management of ranulas. J Oral Maxillofac Surg. 2005; 63:51-4. [ Özet ]
13) Crysdale WS, Mendelsohn JD, Conley S. Ranulas mucoceles of the oral cavity: experience in 26 children. Laryngoscope. 1988; 98:296-8. [ Özet ]
14) Choi TW, Oh CK. Hydrodissection for complete removal of a ranula. Ear Nose Throat J. 2003; 82:946-7, 951. [ Özet ]