


LINGUAL THYROID
Summary
Lingual thyroid is an uncommon embryological aberration characterized by the presence of thyroid tissue located in a site different from the pretracheal region as in normal. Lingual thyroid is the most frequent ectopic location of the thyroid gland, although its clinical incidence varies between 1:3000 and 1:10000. We present a case of a 19-year-old female who presented with severe dysphagia caused by a mass located on the base of the tongue in midline and underwent surgery by using the transhyoid approach.Introduction
Lingual thyroid is thyroid tissue which remains between circumvallate papillae and epiglottis in the root of tongue [1,2]. It is a rare embryologic migration deficiency [2]. Lingual thyroid is located usually in the midline at the base of the tongue [3].It has been reported that the incidence varies from 1:30000 to 1:100000 [1,4]. A postmortem study revealed that in 10% of the cases, thyroid tissue was observed at the base of tongue on macroscopic or microscopic examination [1]. As in the other pathological conditions of the thyroid gland, lingual thyroid is frequently seen in females (80%) [2].
In this report we present a case of symptomatic lingual thyroid and discuss the treatment options with the relevant literature.
Case Presentation
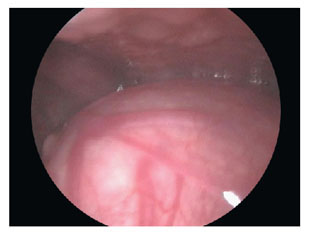
A nineteen-year old woman presented to our clinic with a two-year history of difficulty in swallowing, hoarseness and a foreign body sensation in the throat.On physical examination, there was a mass covered with smooth mucosa, located on the base of the tongue, filling the vallecula and extending to hypopharynx. (Figure 1)
 Büyütmek İçin Tıklayın |
Figure 1: Preoperative endoscopic view |
On ultrasonography of the neck there was no echogenicity suggestive of thyroid gland in its original anatomical location, however there was an echogenicity of a complex cystic formation in the base of the tongue. The mass was 4cm. in diameter and had well defined contours. The center of the mass consisted of cystic degenerative structures.
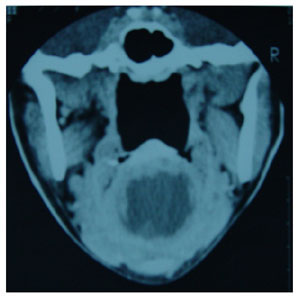
On CT of the neck, there was a well-defined mass with regular contours. The mass was 3x4 cm in length and showed a homogenous contrast enhancement in its adjacent structures and hypodensity in its central part, spreading nearly to the entire mass. It did not invade into any structures or spaces, but it had compression on the adjacent anatomical structures. In fact, when pressure was applied on the anterior of the neck, the mass caused obstruction in the air passage at the level of epiglottis. The mass also extended to the thyroid cartilage. (Figure 2)
 Büyütmek İçin Tıklayın |
Figure 2: CT view of the case |
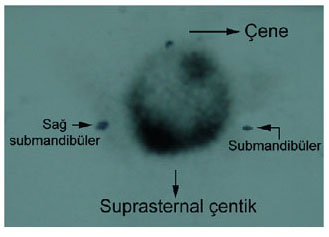
On thyroid scintigraphy, performed fifteen minutes after the intravenous injection of 3 mCi Tc-99 pertechnetate, there was no contrast enhancement suggestive of an activity of the thyroid gland in the location where the gland should be, but there was a hyperactive nodule at the sublingual level including hypoactive regions due to formation of necrosis. (Figure 3)
 Büyütmek İçin Tıklayın |
Figure 3: Preoperative scintigraphic view |
Biochemical analysis showed that TSH was 7.41uIU/ml (normal range: 0.270-4.20) and that FT4 was 1.04ng/dl (normal range: 0.932-1.71) and FT3 was 3.94pg/ml (normal range: 1.82-4.62). Other laboratory investigations were within normal levels.
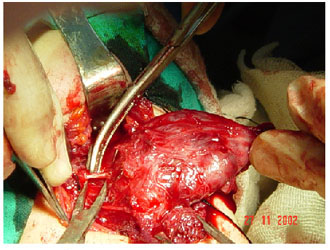
The mass was removed by using transhyoid approach under general anesthesia. The patient was given thyroid hormone replacement postoperatively. (Figure 4,5)
 Büyütmek İçin Tıklayın |
Figure 4: Intraoperative view |
 Büyütmek İçin Tıklayın |
Figure 5: Specimen |
Histological examination of the mass revealed thyroid tissue consisting of follicles filled with colloid in various sizes and degenerative tissue consisting of fibrosis and bleeding centers with an overlying stratified squamous epithelium.
One month after the operation, TSH was 0.053uIU/ml, FT4 2.39ng/dl and FT3 4.24pg/ml.
Six months after the operation, the patient had no complaints and the mass was not visible (Figure 6). On thyroid scintigraphy, performed fifteen minutes after the intravenous injection of 3 mCi Tc-99m pertechnetate, there was no contrast enhancement suggestive of thyroid activity in the region either the thyroid lobes should be present or in the sublingual region (Figure 7). The patient is still being followed by Otolaryngology and Endocrinology clinics.
 Büyütmek İçin Tıklayın |
Figure 6: Postoperative endoscopic view |
 Büyütmek İçin Tıklayın |
Figure 7: Postoperative scintigraphic view in the 6th month |
Discussion
During embryonic life, thyroid gland starts to develop as an endodermal diverticulum between the first and the second pharyngeal pouches and in the ventral and the midline of pharynx. When lobules are formed, the new structure connects to the base of the pharynx through thyroglossal ductus. The primitive thyroid gland developing in the base of the tongue passes infront of the hyoid bone after the migration of the heart and the main vessels into the caudal side. In the seventh embryonic week, the gland settles in front of the trachea [1,3,5].Incomplete caudal migration of the gland may lead to lingual thyroid as a developmental anomaly. [1]. Macroscopic and microscopic examinations show lingual thyroid in 10% of humans,. The disease rarely causes symptoms unless the size of the gland increases [2]. However, the increase in the size of lingual thyroid tissue frequently causes symptoms when there are endocrine changes such as puberty, pregnancy and menstruation [1,3]. Therefore, lingual thyroid is seen seven times more in women than in men [3,6].
Clinical presentation and the severity of the disease are directly related to the size of lingual thyroid tissue. The initial signs of the presentation are disphagy, disphony, dispnea, otalgia and sometimes bleeding from superficial ulcerations [1,7].
The only functional thyroid tissue is lingual thyroid in 70% of patients [8]. Hypothyroidism appears in 33% of cases in various degrees, especially in the young patients, and normal thyroid tissue cannot be detected in 70% of cases [3,8].
There have been 27 cases of lingual thyroid reported in the literature [8].
When physical examination reveals a mass in the base of the tongue and between the epiglottis and circumvallate papillae in the midline, scintigraphy should be performed in the first line. Presence of radioactive iodine enhancement confirms lingual thyroid tissue [1]. Since lingual thyroid is a rare condition, there is no standard treatment protocol. It is commonly agreed that when a mass has been observed at the base of the tongue suggesting lingual thyroid tissue, scintigraphy of the thyroid gland, radiological and laboratory investigations should be performed in order to find if there is a functional thyroid gland apart from lingual thyroid [1].
Surgery is indicated when the disease causes a marked obstruction in the upper respiratory tract and the digestive system and also complications such as ulceration, bleeding or rapidly growing mass, suggesting malignant transformation. Various surgical approaches have been recommended. Transoral approach has been reported to be the most frequently used one [1, 9]. However, authors do not completely agree that the lesion could be totally removed when there is profuse bleeding, even it may not be possible to control bleeding [1]. Another approach is lateral pharyngotomy which is useful only in the treatment of lesions located in the posterior wall or lateral walls of hypopharynx. It provides a wide exposure compared to transoral approach. Another approach is transhyoid which is more advantageous than the other two approaches in that it provides wider and a direct exposition through the midline.
In cases in which the only functional thyroid tissue is lingual thyroid, hypothyroidism may develop when total excision is performed. Therefore, synthetic levo-thyroxin should be administered postoperatively.
Reference
1) Bilgen C, Kirazlı T, Kesimli H, Yavuzer A. Transhyoid approach for lingual thyroid: a case report. KBB İhtisas Dergisi 2001;8(3):238-241
2) Plantet MM, Banal A, Pallud C, Talma V. Infected ossified lingual thyroid goitre. Eur J Radiol. 1997 May;24(3):230-6. [ Özet ]
3) Kutlu R. Kalcioglu T, Baysal T, Sigirci A.(2002) Lingual Thyroid: a case report. [ PDF ]
4) Buckland RW, Pedley J. Lingual Thyroid- A threat to the airway Anaesthesia. 2000 Nov;55(11):1103-5. [ Özet ]
5) Oppenheimer R. Lingual thyroid associated with chronic cough. Otolaryngol Head Neck Surg. 2001 Oct;125(4):433-4. [ Özet ]
6) Basaria S, Westra WH, Cooper DS. Ectopic lingual thyroid Masquearading as Thyroid Cancer Metastases. J Clin Endocrinol Metab. 2001 Jan;86(1):392-5. [ Özet ]
7) Winslow CP, Weisberger EC. Lingual thyroid and neoplastic change: A rewiew of the literature and description of a case. Otolaryngol Head Neck Surg 1997 Dec; 117(6):100-2. [ Özet ]
8) Zoller DC, Silverman BL, Daaboul JJ. (2000) Picture of the month: Lingual thyroid. Arch Pediatr Adolesc Med. 2000 Aug;154(8):843-4. [ Özet ]
9) Akyol M, Ozcan M. Lingual Thyroid. Otolaryngol Head Neck Surg 1996 Nov; 115(5): 483-4. [ Özet ]