


CLINICAL AND RADIOLOGICAL FEATURES OF RHINOLITH: A RARE ENTITY DIAGNOSIS IN 42 PATIENTS
2İstanbul Rumeli Üniversitesi, Odyometri, İstanbul, Turkey
Summary
Introduction: Rhinoliths is a rare entity that can be observed at any age and may have many different presentations, which may cause confusion in differential diagnosis. Rhinoliths are foreign bodies of endogenous or exogenous origin located in the nasal cavity. Malodor nasal discharge, bad breath, nasal obstruction are the most common complaints.The aim of this study is to examine the ages, gender, complaints, and additional pathologies of patients with rhinoliths and to evaluate the characteristics of rhinolith disorders in the light of the literature.
Methods: Patients diagnosed with rhinoliths in an education and research hospital between January 2010 and December 2019 were included in our study. The patients were evaluated retrospectively.
Age, gender, complaints, physical examination findings, radiological results, rhinolith side and localization, rhinolith-related pathologies and treatments were recorded. The characteristics and presentation of rhinolith disease were investigated by evaluating the obtained data.
Results: Of the 42 patients included in our study, 19 were male and 23 were female. The mean age of patients was 24.1 ± 10.7 years (min: 7, max: 44).
In 26 patients (61,9%), rhinoliths was localized in the right nasal cavity and in 16 (38,1%) patients in the left nasal cavity. The most common complaints were nasal obstruction and purulent discharge with malodors. The most common associated pathologies were sinus pathologies (50.1%) and septum deviation (38.1%).
Rhinoliths were removed endoscopically in all patients, 28 of the patients underwent general anesthesia during the procedure, 9 of them were sedoanelgesia and 5 of them were local anesthesia.
Conclusions: A rare case, rhinolith should be strongly considered as differential diagnosis in cases such as unilateral purulent discharge and nasal mass.
Introduction
Rhinolith is a salt minerals-surrounded stone formed by exogenous and endogenous factors in the nasal cavity. In fact, it is very rare disorders in public. It should be considered in case of nasal discharge and unilateral nasal obstruction with malodor, which does not respond to treatment for a long time [1,2]. Rhinolith formation begins with the formation of nidus and the triggering factor may be endogenous (none fragment, exotic dental tissue epidermal debris etc.) or exogenous origin (fruit seed, stones, pieces of paper, buttons, etc.). With Nidus formation, mineralization begins, and a hard capsule is formed, which erodes the nasal mucosa and causes inflammation. Rhinoliths causes nasal discharge with malodor, nasal congestion and sinus problems [3-5].Although rhinolith is thought to be related to low socioeconomic conditions, large rhinolith series are observed in developed countries. Rhinolith, whose incidence varies from country to country, can be observed in all age groups [6,7].
In this study, it was aimed to show the specific symptoms of rhinolith, a rare disease whose diagnosis can be delayed or missed, and to investigate effective treatment methods.
Methods
A total of 42 patients, who were operated for rhinolith between January 2010 and December 2019 in an education and research hospital department of otorhinolaryngology were examined retrospectively.We recorded patients at age, gender, symptoms (nasal obstruction, purulent rhinorrhea, nasal malodor, oral malodor, facial pain, epistaxis), rhinolith side (left nasal cavity, right nasal cavity),rhinolith localization (between the inferior turbinate-nasal septum, middle turbinate and nasal septum or inferior turbinate and middle turbinate) and also identified presence of nidus, associated pathologies with rhinolith (septum deviation, nasal polyp, sinusitis?etc.), the type of surgery used to remove rhinolith (local or general). Medical records, operation notes and radiological examinations were checked to find out that additional sinus surgery was needed.
Our study was conducted in accordance with the principles of the Helsinki Declaration and was approved by our institutional review board (29.04.2020/2020-50). Anterior rhinoscopy and rigid nasal endoscopy and radiological examinations were used in all patients for diagnosis and localization of the rhinolith. In operating room, all patients were treated with endoscopic surgical removal of the rhinolith. The removed rhinolith material was sent for pathological examination.
Statistical Analysis
SPSS 15.0 for Windows program was used for statistical analysis. Descriptive statistics; number and percentage for categorical variables, mean, standard deviation, minimum, maximum for numerical variables. Since the numerical variable provided the normal distribution condition, comparisons of two independent groups were made by Student's t test. The ratios in the groups were compared by Chi-Square Analysis. Statistical significance level of alpha was accepted as p <0.05.
Results
In our study, there were 19 male and 23 female patients who were diagnosed and operated with rhinolith. The mean age of the patients was 24,1±10,7 years (min: 7, max:44). When the patients were divided into two age groups; ?30 years and ?30 years, we observed that most patients were in the <30 age group (66.7%). 11of 42 patients had no radiological examinations.The rhinolith was localized in the right nasal cavity in 26 patients (61,9%), and in the left nasal cavity in 16 patients (38,1%).The most common localization of the rhinolith was the inferior turbinate and the nasal septum(n=29).The distribution of the localization of rhinolith is shown in table 1. Nasal obstruction (71,4%), purulent rhinorrhea and nasal malodor were the most common complaints. In addition, epistaxis was determined in 7 patients (16,7%), headache and facial pain in 7 patients (16,7%). (Table 1)
){kind=link}
Table 1: Patient demographics and rhinolith characteristics
One patient had history of a foreign body inside her nose. After removal of rhinolith, nidus was determined in 3 patients (7,1%), one of which was the fruit seed and the other two were buttons.
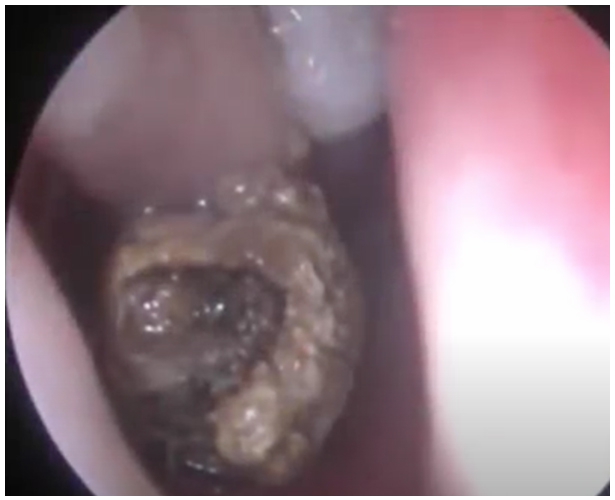
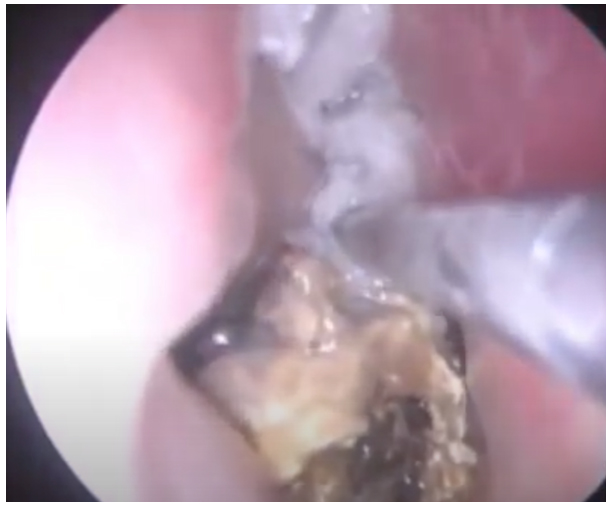
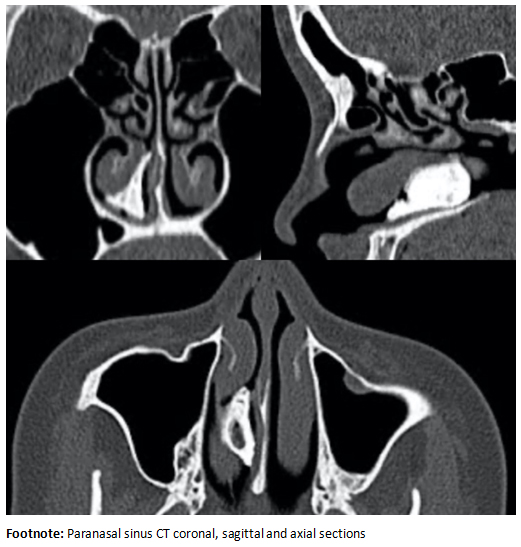
We evaluated the relation between the rhinolith and other sinonasal structures with rigid endoscopy (Figure 1), CT images and operation notes. Sinus pathology (50,1%) was most common accompying sinonasal pathological finding (Figure 2). These sinus pathologies were mucosal thickening in the maxillary sinus(n=16), retention cyst in the maxillary sinus(n=2), polyp in the maxillary sinus(n=1), complete opacification of the maxillary sinus (n=2).All the sinus pathologies were at the same side with rhinolith. The second concomitant sinonasal pathological finding was septum deviation (38,1%). In 13 patients, the septum deviations were in the opposite side of the nasal cavity where the rhinolith was present (Figure 3).
All patients were operated on under operating room conditions. General anesthesia was performed in 28 (66.7%) patients, sedation in 9 (21.4%) patients, and local anesthesia in 5 patients (11.9%).
 Büyütmek İçin Tıklayın |
Figure 1: Rigid Nasal Endoscopy Image of Rhinolith in The Nasal Passag |
 Büyütmek İçin Tıklayın |
Figure 2: Rhinolith causing purulent sinus discharge in the nasal passage |
 Büyütmek İçin Tıklayın |
Figure 3: Rhinolith Paranasal Sinus CT Image |
Discussion
Rhinolith formation is one of the rare entities. Despite this, the incidence of male and female gender does not change and is a disorder observed at all age. Yildiz et al. In their study, the percentage of female included was 58.3% and the percentage of male was 41.7%. The ages of the patients included in the study were observed as min 2 and max 62 years [8]. In a study conducted by Akkoca et al., no statistical difference was found between gender, age and frequency of rhinolith [9]. In another study, the ratio of female to male was 4: 1 and no difference was found in the ages of the patients [10]. In our study, the percentage of female patients was 54.74% and the percentage of men was 45.24%. Ages were evaluated as minimum age 7 and maximum 44 years. In the studies in the literature, no significant differences were found between the ages and genders of similar patients. It is caused by the wide etiology of rhinolith and can be observed in many age groups due to its many causes of endogenous and exogenous.Patients with rhinoliths most frequently complain of unilateral nasal congestion, purulent discharge, facial pain, nasal / oral malodor [10]. Ozdemir et al. In their study, the most common complaint was purulent nasal discharge and nasal obstruction. Aksakal et al. In their study, the most common complaint is nasal obstruction followed by nasal discharge and facial pain, respectively [5,10]. In our study, the most common complaint was nasal obstruction (71.4%), nasal discharge and nasal malodor. In addition, 7 patients had epistaxis (16.7%) and 7 patients had headache and facial pain (16.7%). There are many case reports about rhinolith in the literature. Apart from common complaints, there are studies showing that rhinolith may cause severe symptoms that cause septal perforation due to inflammation, as well as sinusitis and its complications to progress to the intracranial area [11,12]. Long rhinoliths formation process and patients being asymptomatic during this process may explain the pathophysiology of severe complicated cases. Since rhinoliths can cause severe complications, rigid nasal endoscopy is recommended from nasal discharge that do not respond to antibiotic therapy [2].
In this study, rhinolith was removed in 3 of our patients, after which nidus formation was detected. Fruit seeds were found in one patient, and buttons were found in two patients. Özdemir et al. In their study, it was observed that they obtained similar results [5]. There is a nidus formation that can occur for many different reasons. In the literature, there are studies especially teeth fragment with nidus origin, which are defined as endogenous nidus [13,14].
In the literature, studies on rhinolith, no correlation was found between the presence of rhinolith and the nasal cavity side. Akkoca et al. In their study, 11 of the rhinolith localization was found on the left and 7 on the right side [9]. Ozdemir et al. In their studies, 11 rhinoliths were reported to be left side and 10 to right side [5]. In current study, 26 (61.9%) patients had rhinolith in the right-side nasal cavity and 16 (38.1%) patients had rhinoliths in the left-side nasal cavity. The reason for the larger number of rhinoliths in the right-side nasal cavity may be exogenous rhinoliths. The fact that the dominant hand is usually the right hand may contribute to this situation.
There may be many pathologies that accompany rhinoliths. Some of these pathologies (inferior turbinate hypertrophy, septal deviation, etc.) can prevent the rhinolith from appearing on physical examination and delay the diagnosis of rhinoliths. In patients with chronic sinusitis, the severity of rhinoliths symptoms may increase [9]. Therefore, rigid and flexible nasal endoscopy is recommended in addition to anterior rhinoscopy during physical examination [15]. In addition, there are publications showing computed tomography (CT) is useful for differential diagnosis with benign and malignant tumors [2,16]. İn current study, it was observed that the most common complaint was sinus pathology as a result of CT image images (mucosal thickening in the maxillary sinus, retention cyst in the maxillary sinus, polyp in the maxillary sinus, complete opacification of the maxillary sinus). If our patients had sinus pathology, they were on the same side as rhinoliths. This suggests that rhinolith may trigger sinus pathologies. The second accompanying pathology was septum deviation (38.1%). The septum deviations were in the opposite side of the nasal cavity where the rhinolith was present (n=13).
In most cases, it is removed endoscopically, and post-surgical antibiotics are recommended. Some complicated cases may require more advanced techniques [17]. In our study, all patients were removed rhinolith endoscopically. General anesthesia was used in 32 patients (88.1%), and local anesthesia was used in 5 patients (11.9%).
Reference
1) Hadi U, Ghossaini S, Zaytoun G. Rhinolithiasis: a forgotten entity. Otolaryngol Head Neck Surg 2002;126:48-51. [ Özet ]
2) Yuca K, Caksen H, Etlik O, Bayram I, Sakin YF, Dülger H, et al. The importance of rigid nasal endoscopy in the diagnosis and treatment of rhinolithiasis. Auris Nasus Larynx 2006;33:19-22. [ Özet ]
3) Varadharajan K, Stephens J, Madani G, Parikh A. Rhinolith causing unilateral chronic maxillary rhinosinusitis. BMJ Case Rep. 2014;17. [ Özet ]
4) Zalagh M, Akhaddar A, Benariba F. Chronic rhinorrhea revealing an actinomycotic rhinolithiasis with ectopic tooth. Int J Oral Maxillofac Surg 2012;41:297-9. [ Özet ]
5) Ozdemir S, Akbas Y, Gorgulu O, Selcuk T, Sayar C. Rhinolithiasis: review of 21 cases. Am J Rhinol Allergy 2010;24:136-9. [ Özet ]
6) Cheng CC, Fang TJ, Lee LA, Li HY, Kuo YL, Chen TM. Rhinolith from a plastic object in the nasal cavity for more than 20 years. Pediatr Int 2011;53:135-6. [ Özet ]
7) Saibene AM, Bebi V, Borloni R, Felisati G. Rock, paper, endoscopy: a baffling case of rhinolith. BMJ Case Rep 2013;9. [ Özet ]
8) Yildiz E, Kuzu S, Ulu S, Kahveci OK, Gunebakan C, Bucak A. Rhinoliths: Analysis of 24 Interested Forgotten Foreign Body Cases. Ear Nose Throat J 2020;13. [ Özet ]
9) Akkoca O, Tuzuner A, Demirci S, Unlu C, Uzunkulaoglu H, Arslan N, et al. Patient Characteristics and Frequent Localizations of Rhinoliths. Turk Arch Otorhinolaryngol 2016;54:154-7. [ Özet ]
10) Aksakal C. Rhinolith: Examining the clinical, radiological and surgical features of 23 cases. Auris Nasus Larynx 2019;46:542-7. [ Özet ]
11) Kharoubi S. Rhinolithiasis associated with septal perforation. A case report. Acta Otorhinolaryngol Belg 1998;52:241-5. [ Özet ]
12) Atmaca S, Belet N, Sensoy G, Belet U. Rhinolithiasis: an unusual cause of sinusitis complicated with frontal osteomyelitis and epidural abscess. Turk J Pediatr. 2010;52:187-90. [ Özet ]
13) Janardhan N, Kumar SR, Reddy RR, Kumar CA. Rhinolithiasis due to supernumerary ectopic tooth: very rare case. Indian J Otolaryngol Head Neck Surg 2013;65:383-4. [ Özet ]
14) Dalben Gda S, Vargas VP, Barbosa BA, Gomide MR, Consolaro A. Intranasal tooth and associated rhinolith in a patient with cleft lip and palate. Ear Nose Throat J 2013;92:10-4. [ Özet ]
15) Ayub ur R, Muhammad MN, Moallam FA. Endoscopy in rhinolithiasis. J Coll Physicians Surg Pak 2012;22:601-3. [ Özet ]
16) Flood TR. Rhinolith: an unusual cause of palatal perforation. Br J Oral Maxillofac Surg 1988;26:486-90. [ Özet ]
17) Sofferman RA. The septal translocation procedure: an alternative to lateral rhinotomy. Otolaryngol Head Neck Surg 1988;98:18-25. [ Özet ]