


THREE- DIMENSIONAL MORPHOMETRIC EVALUATION OF ANTERIOR EPITYMPANIC RECESS AND COG PROCESS IN TEMPORAL BONES WITH PETROUS APEX PNEUMATIZATION
2Balıkesir Üniversitesi, Tıp Fakültesi, KBB ABD, Balıkesir, Turkey
Summary
Purpose: To assess the association of petrous apex pneumatization with Cog process length and anterior epitympanic recess volume using 3- dimensional reconstructed computerized tomography sections of the temporal bone, in this cross- sectional, radio-anatomical investigation.Method: We measured anterior epitympanic recess volumes from three- dimensional models reconstructed on OsiriX software. The comparisons of Cog process lengths and anterior epitympanic recess volumes of the temporal bones with and without petrous apex pneumatization were performed.
Results: Cog process length was significantly lower, and AER volume was significantly higher in temporal bones with petrous apex pneumatization compared to the bones without (p=0.01 and p<0.001, respectively).
Conclusion: Pneumatization of petrous apex was found associated with a wider AER and shorter Cog process that might bring about a physiological advantage against retraction pocket development because of well- pneumatized epitympanum.
Introduction
Various anatomical structures in the temporal bone may have developmental associations having both surgical and clinical implications. Because of the similar embryologic origin, the shape, deepness and/or volume of the spaces like the sinus tympani and anterior epitympanic recess (AER) might be influenced by the aeration of the mastoid and the petrous apex [1]. Additionally, development of Cog process may also have an association with the aeration of the mastoid and petrous apex. In the temporal bones with a wider AER and shorter Cog process, epitympanum might be well -pneumatized, in association with decreased risk of retraction pockets. Moreover, the temporal bones with decreased AER volume and longer Cog process might present with a Korner's septum, bringing about an increased complication risk [2]. Thus, pneumatization of petrous apex might be associated with the development of several anatomic structures in the temporal bone, having many surgical and clinical implication. In this aspect, the goal of this study was to assess the association of petrous apex pneumatization with the length of Cog process and the volume of AER using 3- dimensional (3D) reconstructed computerized tomography (CT) sections of the temporal bone, in this cross- sectional, radio-anatomical investigation.Methods
Subjects, measurements, and designBefore the initiation of the search for the temporal bone CT sections with pneumatized petrous apex, the local ethical committee approved the study. This retrospective, cross- sectional, 3D radio-anatomical study was conducted in accordance with Helsinki Declaration by World Medical Association. From the institutional radiologic archive of our tertiary center, we identified 65 temporal CT sections from 36 patients with petrous apex pneumatization, and 60 temporal bones from 30 patients without any petrous apex pneumatization on any side between May 2019 and May 2020. The patients with an earlier trauma history, chronic otitis media, temporal bone/ear surgery history and cholesteatoma were not included in the study. We used a 16-slice CT unit (Siemens, Germany) together with a Picture Archiving Systems (PACS) (Akgun, Turkey) for compiling images to be reconstructed in 3D. The CT scanner had following parameters: 0.8-s rotation time, 1.2 mm slice thickness, 1 mm pitch, and 130 kVp.
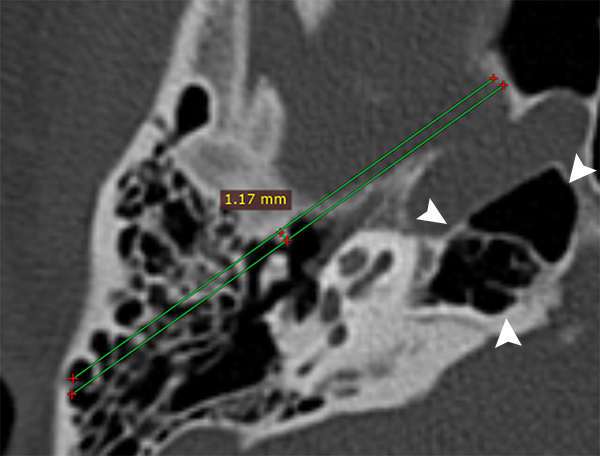
Using the OsiriX v3.8.1 software for Mac-OS (Pixmeo SARL, Switzerland), a six year- experienced radiologist performed measurements of the volume of AER using the volumetric function of OsiriX, and of Cog process length (Fig 1). Measurement of the volume of AER was based on the manual segmentation protocol. In serial slices tracing the borders of the recess, the area was measured and multiplied by the slice thickness. On all temporal CT sections, a 3D diagram of the AER was created to calculate the volume of AER (mm3). Both 3D reconstructions and measurements were performed twice with an interval of 6 weeks to assess intra-observer agreement. Considering the presence of pneumatized petrous apex, we formed two groups: the pneumatized petrous apex group (temporal bones with petrous apex pneumatization were included) and the control group (temporal bones without petrous apex pneumatization were included from the patients without any petrous apex pneumatization on any side). The length of Cog process and the volume of AER were statistically compared between these groups.
 Büyütmek İçin Tıklayın |
Fig 1: Measurement of Cog process length on temporal bone image with petrous apex pneumatization (arrowheads). |
Statistical Analysis
Results of continuous data were presented as mean± SD, and of sequential data were presented as median (min-max). Kolmogorov- Smirnov normality test was used to assess the data distribution. The data of age did not distribute normally, thus comparison was performed using Mann Whitney U test. The data of Cog process length and AER volume did distribute normally, thus comparisons were performed using independent samples T test. Comparison of gender distribution of the groups was performed using Chi square test. Statistical analysis was performed on SPSS v23.0 for Mac-OS 11 (SPSS Inc., Chicago, IL, USA). P<0.05 was considered the level of statistical significance.
Results
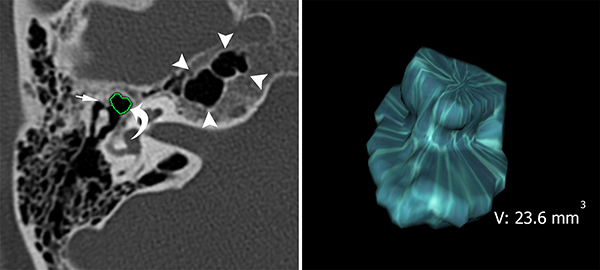
In total, 66 patients underwent a temporal bone CT were included in the study. Thirty-six patients with pneumatized petrous apex [18 females-18 males with a median age of 38 (10-78) years] and 30 other patients without pneumatized petrous apex [15 females-15 males with a median age of 40 (11-72) years] were eligible. The gender distribution and the median age of the groups were not different (p=1 and p=0.934, respectively).Petrous apex pneumatization group consisted of 65 temporal bone sections with a pneumatized petrous apex from 36 patients [7 (19.4%) patients with unilateral, and 29 (80.6%) patients with bilateral pneumatization], and the control group consisted of 60 temporal bones from 30 patients without petrous apex pneumatization on any side. The mean AER volume and Cog process length of the groups were presented in Table 1. The mean AER volume was significantly higher, and the mean Cog process length was significantly lower in temporal bones with petrous apex pneumatization (Fig 2), compared with the patients without (Fig 3) (p<0.001).
){kind=link}
 Büyütmek İçin Tıklayın |
Fig 2: A 30-year-old man with petrous apex pneumatization (arrowheads). Anterior epitympanic recess volume was measured with tracing borders (curved arrow) of the recess in serial slices (A) and 3D- volume diagram of anterior epitympanic recess was created (B). Cog process identified by thin arrow. |
 Büyütmek İçin Tıklayın |
Fig 3: Measurement of anterior epitympanic recess (curved arrow) in a temporal bone without petrous apex pneumatization (arrowheads). Cog process was identified by thin arrow. |
Discussion
Compiling data from 3D reconstructed CT images of the patients with petrous apex pneumatization, we investigated the cross -sectional, radio- anatomical association of pneumatized petrous apex with AER and Cog process in this retrospective study. Although radiologic investigations are not capable of reflecting the real anatomy completely, our 3D reconstructed models provided realistic sections, and opportunity of measuring AER volume, in keeping with earlier publications [1-3]. Our results showed that temporal bones with pneumatized petrous apex had a wider AER and shorter Cog process. Thus, we can hypothesize that petrous apex pneumatization might bring about a physiological advantage against retraction pocket development because of well- pneumatized epitympanum and shorter Cog process.Although various otologic symptoms were reported in patients with abnormal petrous apex aeration [4], the clinical and surgical importance of petrous apex pneumatization is not clear. In the study by Stieglitz et al, petrous apex pneumatization was reported as a risk factor cerebrospinal fluid leak after schwannoma surgery [5]. Additionally, in the prior literature of English- language, there exist several studies conducted on the various lesions of petrous apex [6-8]. The association of benign lesions like cholesteatoma and cholesterol granuloma with petrous apex pneumatization was previously reported [9,10]. Petrous apex pneumatization is known as an anatomic variant that may be both symmetric and asymmetric, as we found that the rate of bilateral petrous apex pneumatization was 80.6% in our study group. However, the anatomic and physiologic factors affecting the pneumatization pattern of petrous apex are not clear. Hence, in keeping with previous investigations, we hypothesize that pneumatization of petrous apex might have a developmental association with air- filled spaces of the temporal bone, including mastoid air cells [4,11], sinus tympani [1] and epitympanum. Moreover, Hentona et al [11]. suggested to take petrous apex pneumatization into consideration in the studies focusing on the volume of middle ear. In our study, we also measured the length of the Cog process, considering as an obstacle against the aeration of epitympanum. Our results showed that temporal bones with petrous apex pneumatization were associated with a shorter Cog process and a wider AER.
This study simply presents cross- sectional, radio- anatomical associations of petrous apex pneumatization using a computer -assisted quantitative 3D method, with some limitations. Embryological mechanism of the associations remained unclear because of the retrospective and cross-sectional characteristics of the study. Additionally, as being a radiologic investigation, it might not completely reflect the real anatomy as a cadaveric dissection study or a histopathologic temporal bone study [12]. Nevertheless, 3D reconstruction method has an advantage against conventional methods, for the studies on the anatomy of air- filled spaces of the temporal bone.
Conclusion
Pneumatization of petrous apex was found associated with a wider AER and shorter Cog process that might bring about a physiological advantage against retraction pocket development because of well- pneumatized epitympanum.
CONFLICT OF INTEREST STATEMENT
The authors declare that there is no conflict of interest.
FINANCIAL DISCLOSURE
The authors declared that this study has received no financial support.
Reference
1) Bekci T, Hizli O, Ozturk M, Yildirim G. Quantitative three-dimensional computed tomography analysis of sinus tympani volume in temporal bones with petrous apex pneumatization. Auris Nasus Larynx 2020; 47: 587-592. [ Özet ]
2) Hizli O, Bekci T, Aslan S. Anterior epitympanic recess volume and Cog process length in temporal bones with Körner's septum: A radio- anatomical investigation. Auris Nasus Larynx 2021. [ Özet ]
3) Hizli O, Ozturk M, Bekci T, Yildirim G. Sinus tympani volume in temporal bones with körner's septum: A quantitative three-dimensional analysis. KBB-Forum 2019; 18: 300-304. [ 4) Yetiser S, Kertmen M, Taser M. Abnormal petrous apex aeration. Review of 12 cases. Acta Otorhinolaryngol Belg 2002; 56: 65-71. [ Özet ]
5) Stieglitz LH, Giordano M, Gerganov V, Raabe A, Samii A, Samii M, Lüdemann WO. Petrous bone pneumatization is a risk factor for cerebrospinal fluid fistula following vestibular schwannoma surgery. Neurosurgery 2010; 67: 509-515. [ Özet ]
6) Hodges J, Matsumoto J, Jaeger N, Wispelwey B. Gradenigo's Syndrome and Bacterial Meningitis in a Patient with a Petrous Apex Cholesterol Granuloma. Case Rep Infect Dis 2020; 2020: 8822053. [ Özet ]
7) Verma RR, Kumar R, Sagar P, Kumar R. Endoscopic Transsphenoidal Drainage of Petrous Apex Mucocele. Ear Nose Throat J 2020; 145561320984997. [ Özet ]
8) Radhakrishnan R, Son HJ, Koch BL. Petrous apex lesions in the pediatric population. Pediatr Radiol 2014; 44: 325-339; quiz 323-324. [ Özet ]
9) Connor SE, Leung R, Natas S. Imaging of the petrous apex: a pictorial review. Br J Radiol 2008; 81: 427-435. [ Özet ]
10) Razek AA, Huang BY. Lesions of the petrous apex: classification and findings at CT and MR imaging. Radiographics 2012; 32: 151-173. [ Özet ]
11) Hentona H, Ohkubo J, Tsutsumi T, Tanaka H, Komatsuzaki A. [Pneumatization of the petrous apex]. Nihon Jibiinkoka Gakkai Kaiho 1994; 97: 450-456. [ Özet ]
12) Monsanto RD, Pauna HF, Kaya S, Hızlı Ö, Kwon G, Paparella MM, Cureoglu S. Epitympanum volume and tympanic isthmus area in temporal bones with retraction pockets. Laryngoscope 2016; 126: E369-e374. [ Özet ] ![]() Tam Metin ]
Tam Metin ]