


CAROTID BLOWOUT SYNDROME DURING RADIOTHERAPY: A CASE PRESENTATION AND REVIEW OF A RARE ENTITY
2Hacettepe, Radyasyon Onkolojisi, Ankara, Türkiye
Summary
Carotid blowout syndrome (CBS) is an uncommon but a potentially lethal complication with 40% mortality and 60% morbidity, encountered in head and neck cancer patients. CBS has three subtypes; threatened, impending, acute. Impending form is characterized by spontaneously resolving recurrent epistaxis attacs. Radical neck dissection, pharyngocutaneous fistulae, recurrent/ residual tumor and irradiation have been determined as potential risk factors of CBS. Nasopharyngeal carcinoma is highly radiosensitive and its primary treatment is radiotherapy. We report a 77-year-old male patient with T4N2cM0 nasopharyngeal cancer with impending form of CBS diagnosed during the initial days of radiation.Introduction
Carotid blowout syndrome (CBS) is a life- threatening condition which is defined as rupture or exposure of carotid artery.[1,2] It is a potentially lethal complication in patients with head and neck cancer. CBS has an average mortality rate of 40 % and morbidity rate of 60%.[3,4] Radical neck dissection, pharyngocutaneous fistulae, irradiation, recurrent or residual tumor have been implicated as potential causes of CBS.[3-6] Nasopharyngeal cancer is a radiosensitive tumor and the primary treatment is radiotherapy with or without chemotherapy depending on the stage.[5,7] Although radiation induced CBS with pseudoaneurysm formation is an uncommon complication in nasopharyngeal cancer, several reports had declared cases with pseudoaneurysm of petrous segment of internal carotid artery.[1,5,7-10] In this paper, an adult patient who had been on radiotherapy due to nasopharyngeal cancer and developed CBS during initialdays of treatement is presented and literature regarded CBS is reviewed.Case Presentation
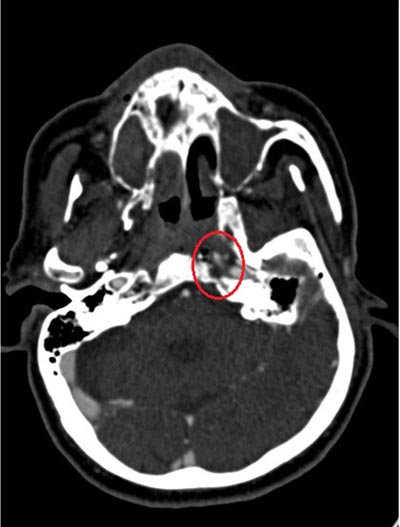
A 77-year old male patient admitted to our clinic with bilateral neck masses. Otolaryngological examination revealed an ulcerative mass on postero-superior wall of nasopharynx, several conglomerated lymphadenopathies on bilateral level II and V and right vocal cord paralysis. From his past medical history, it was learned that he had an ischemic cerebrovascular attack twenty years ago and he has diabetes mellitus type II. Magnetic Resonance Imaging revealed a mass in nasopharynx which was invading cavernous sinus and prevertebral muscles; and there were metastatic cervical lymphadenopathies in level II-III-V bilaterally. Histopathological diagnosis of the nasopharyngeal mass was non-keratinized undifferentiated nasopharyngeal cancer. Patient was diagnosed as T4N2cM0 nasopharyngeal cancer, and concomittant chemoradiotherapy was planned. Seventy Gy with a fraction dose of 2 Gy to gross tumor volume, 66 Gy to whole nasopharynx and positive lymph nodes was planned with intensity modulated radiotherapy technique. Cisplatinium, with a dose of 35 mg/m2/ week, was planned concomitantly with radiotherapy. On the 18th day of radiotherapy, patient admitted to the emergency clinic with epistaxis. He stated that he had several episodes of bleeding all of which resolved spontaneously during the last three days. In the emergency clinic, hemoglobin level was detected to be 8.9 mg/dl. On otolaryngological examination an oozing type epistaxis originating from the nasopharyngeal mass was noticed. The bleeding was controlled with simple transnasal packing. He was hospitalized and two unites of red blood cells were transfused. After the patient was stabilized in hemodynamic means, an angiography with computerized tomography was performed with suspicion of pseudoaneurysm on internal carotid artery wall. It was detected that a 9 mm left internal carotid artery pseudoaneurysm was present with certain amount of extravasation (Figure 1, 2). The patient was consulted with interventional neuroradiology and stenting of the internal carotid artery segment with pseudoaneurysm was planned. Just after the radiological imaging was performed; patient had a profuse epistaxis and he deteriorated rapidly. He had a filliform pulse with remarkable hypotension. He was intubated and resuscitation was started immediately. He was given proper fluid support intravenously and atropine, adrenaline, bicarbonate by close monitoring. Bleeding continued during resuscitation and at the end of an hour patient was accepted as exitus.
 Büyütmek İçin Tıklayın |
Figure 1: Pseudoaneurysm formation on left internal carotid artery, petrocavernous junction (Computed Tomography Angiography). |
 Büyütmek İçin Tıklayın |
Figure 2: Pseudoaneurysm formation on left internal carotid artery, petrocavernous junction (Computed Tomography Angiography). |
Discussion
Carotid blowout syndrome might be observed due to head and neck tumor itself or the treatment modality. Not only a part of carotid artery could be infiltrated by tumor or its neck metastasis; but also it could be nuded or damaged by treatment modalities such as neck dissection or irradiation.[4,11]In the treatment of nasopharyngeal cancer, radiotherapy is being administered to the primary site and neck bilaterally. Large arteries are relatively resistant to radiotherapy however stenosis may be observed even in large vessels following radiotherapy. This side effect is a delayed complication of radiotherapy and is observed years after treatement. Carotid blowout syndrome is a rare complication of radiotherapy and usually occurs after re-irradiation. In a review which was published recently, the rate of CBS was 2.6% for patients receiving salvage head and neck reirradiation.[12] The median time to CBS, which was measured from the begining of reirradiation was 7.5 months. In this review, patients receiving reirradiation with stereotactic body radiotherapy (SBRT) were excluded. The rate of CBS in patients receiving salvage radiotherapy with SBRT is reported to be in the range of 10% to 17%.[13,14] It is observed during 5 to 24 months following SBRT.
Radiotherapy is involved in pathophysiology of CBS as it can lead to vascular pathologies such as obliteration of vaso vasorum, adventitial fibrosis, atherosclerosis, weakening of arterial wall, subendothelial vacoulization, fragmentation of tunica media elastic fibers of the carotid artery.[6,7,10] Irradiation may also cause osteonecrosis of petrosal bone which is critical in formation of pseudoaneurysm at petrosal segment of carotid artery which can trigger CBS.[7,8] Recurrent cases require booster doses of radiotherapy which makes carotid artery, particularly the petrous segment, more vulnerable to pseudoaneurysm formation and further bleeding.[5,7] Our case is unusual, as the damage to the large vessel was seen during the first line radiotherapy, whereas in literature CBS is usually reported with reirradiation or after the conclusion of therapy.[1,2,5,8]
Neck dissection is known as another etiologic factor for CBS. Postoperative complications after neck dissection, such as flap necrosis, wound infection, pharyngocutaneous fistula formation may cause arterial wall damage and injuries of carotid artery.[5,6,15]
Carotid blowout syndrome is classified into three subtypes; threatened, impending and acute. Threatened CBS is defined as exposure of the carotid artery due to wound breakdown or neoplastic invasion of carotid system although hemorrhage has not occured yet. If the carotid artery is not promptly covered with healthy tissue, the rupture is inevitable. Impending CBS is defined as short episodes of bleeding which can resolve spontaneously or can be controlled by simple packing. However complete rupture is certain; only the time is unknown. Acute CBS is defined as profuse bleeding which cannot be controlled by simple packing. As there is a complete and sudden rupture of the carotid artery, patient deteriorates rapidly. Unless the vessel repair is provided immediately, resuscitation would not help for long term stabilization.[1,4,8,16] Regarding the spontaneous recovering recurrent epistxis attacks, our case should be considered as an impending type of CBS with pseudoaneurysm formation.
Management of CBS should depend on some principles; the initial and cardinal priority is to provide both respiratory and cardiac stabilization. The next step should be identification of the site and extent of the pathology via diagnostic angiography. 4 In case of carotid system involvement (internal or common); temporary balloon occlusion test (BTO) should be performed to determine intracranial collateral circulation. The purpose of BTO is to assess the availability of collateral circulation if the ruptured carotid artery is permanently occluded.[2,4] Balloon occlusion test is a decision making step not only for endovascular treatment modalities but also for the open surgery techniques. Emergent surgical ligation of carotid system without BTO has average neurologic morbidity of 60%.[17] Prior to the neck dissection procedure or irradiation of an extended tumor invading carotid system; result of the BTO may help to decide whether to ligate the vessel or to construct a bypass.[6] In literature; endovascular modalities are more preferrable compared to surgical management of CBS. Surgical management is usually difficult as the exploration and repair of previously irradiated fields is annoying.[2,6] On the other hand, endovascular techniques are less invasive. They can be performed with local anesthesia and do not necessitate any tissue harvesting.[3,4,6,16]
Based on the BTO result there are two main types of endovascular treatment; de-constructive versus constructive. Deconstructive management is designed for the patients who can tolerate BTO and are suitable for the permanent occlusion of carotid artery by coil or glue embolization. Constructive management is designed for the patients who can not tolerate BTO therefore for patent and safe arterial flow is provided by endovascular stents.[2,4,11,15] Despite the BTO results, there are certain reports in the literature stating cases who had passed the test however developed ischemic complications including cerebral infarction due to deconstructive embolization procedure. The reason is thought to be that BTO is a short timed- test (20-30 minutes) and sometimes collateral circulation insufficency may be seen in longer period.[8]
In case of nasopharyngeal cancer which is irradiated, CBS is seen as a result of pseudoaneurysm formation mainly in medium to large sized vessels on a basis of atherosclerosis.[7,9,10] Our patient had history of ischemic cerebrovascular attack which gives suspicion of tendency to thrombosis in a retrospective fashion. As sson as pseudoaneurysm is detected on angiography both deconstructive and constructive endovascular modalities can be considered, however each has its own limitations. Pseudoaneurysm is an arterial bulging which is not baring normal vessel wall structure. Besides surrounding bone is usually ostoenecrotic which lacks any support mechanisms. There can be acute rupture of pseudoaneurysm during inflation of BTO balloon or stent replacement.[11] Also after embolization of pseudoaneurysm extravasation of coils has been seen in some cases.[7] To find a solution; coil embolization with stent placement has been worked on, but is been still controversial.[8,18]
Following endovascular procedures, there might be recurrent hemorrhages which are found to be correlated either with infection or anticoagulant therapy. Therefore appropiate antibiotic treatment should be administered after both deconctructive and constructive procedures.[2,15] Anticoagulant therapy is generally started just before stent placement and continued lifelong but much more intensive in the first week. As a precaution, bleeding parameters should be followed intimately, unnecessary medication should be avoided when the optimum level is reached.[2,16]
Carotid blowout syndrome might cause lethal bleeding and it is better to realize risk factors in the earlier period and to intervene if possible. It has been noticed that focal soft tissue necrosis on Magnetic Resonance Imaging of patients with nasopharyngeal cancer is a predictor of CBS.[9] Also both the radiologist and the head neck cancer team (surgeon, oncologist and radiation oncologist) should be alert for pseudoaneurysm formation, vessel wall damages and the degree of adjacent osteonecrosis to predict any possible form of CBS.[1,5]
In conclusion; CBS is an uncommon but lethal complication of head and neck cancer patients. Not only the profuse hemorrhage, but also minimal recurrent bleedings should be examined intimately. Once it occurs, patient should be evaluated immediately and proper treatment should be administered quickly. As it is more important to avoid such a catastrophic complication; predictors on routine imaging techniques should not be missed and fundamental precautions should be applied.
Reference
1) Yanik B, Keyik B, Conkbayir I, Teber MA. Carotid blowout syndrome with oronasal hemorrhage: magnetic resonance imaging findings. Jpn J Radiol 2011 Jan;29(1):72-5. [ Özet ]
2) Wan WS, Lai V, Lau HY, Wong YC, Poon WL, Tan CB. Endovascular treatment paradigm of carotid blowout syndrome: Review of 8-years experience. Eur J Radiol 2013 Jan;82(1):95-9. [ Özet ]
3) Pathak KA, Viallet NR, Nason RW. Sternocleidomastoid muscle interposition to prevent carotid artery blowout. J Surg Oncol 2008 Dec 1;98(7):565-6. [ Özet ]
4) Zussman B, Gonzalez LF, Dumont A, Tjoumakaris S, Rosenwasser R, Hasan D, et al. Endovascular Management of Carotid Blowout: Institutional Experience and Literature Review. World Neurosurg 2012 Jul;78(1-2):109-14. [ Özet ]
5) Luo CB, Teng MM, Chang FC. Radiation acute carotid blowout syndromes of the ascending pharyngeal and internal carotid arteries in nasopharyngeal carcinoma. Eur Arch Otorhinolaryngol 2006 Jul;263(7):644-6.
6) Roh JL, Suh DC, Kim MR, Lee JH, Choi JW, Choi SH, et al. Endovascular management of carotid blowout syndrome in patients with head and neck cancers. Oral Oncol 2008 Sep;44(9):844-50. [ Özet ]
7) Cheng KM, Chan CM, Cheung YL, Chiu HM, Tang KW, Law CK. Endovascular treatment of radiation-induced petrous internal carotid artery aneurysm presenting with acute haemorrhage. A report of two cases. Acta Neurochir (Wien) 2001;143(4):351-5; discussion 355-6. [ Özet ]
8) Auyeung KM, Lui WM, Chow LC, Chan FL. Massive epistaxis related to petrous carotid artery pseudoaneurysm after radiation therapy: emergency treatment with covered stent in two cases. AJNR Am J Neuroradiol 2003 Aug;24(7):1449-52.
9) Chin SC, Jen YM, Chen CY, Som PM. Necrotic nasopharyngeal mucosa: an ominous MR sign of a carotid artery pseudoaneurysm. AJNR Am J Neuroradiol 2005 Feb;26(2):414-6. [ Özet ]
10) Li SH, Hsu SW, Wang SL, Chen HC, Huang CH. Pseudoaneurysm of the external carotid artery branch following radiotherapy for nasopharyngeal carcinoma. Jpn J Clin Oncol 2007 Apr;37(4):310-3. [ Özet ]
11) Chaloupka JC, Putman CM, Citardi MJ, Ross DA, Sasaki CT. Endovascular therapy for the carotid blowout syndrome in head and neck surgical patients: diagnostic and managerial considerations. AJNR Am J Neuroradiol 1996 May;17(5):843-52. [ Özet ]
12) McDonald MW, Moore MG, Johnstone PA. Risk of carotid blowout after reirradiation of the head and neck: a systematic review. Int J Radiat Oncol Biol Phys 2012 Mar 1;82(3):1083-9.
13) Cengiz M, Ozyigit G, Yazici G, Dogan A, Yildiz F, Zorlu F, et al. Salvage reirradiaton with stereotactic body radiotherapy for locally recurrent head-and-neck tumors. Int J Radiat Oncol Biol Phys 2011 Sep 1;81(1):104-9. [ Özet ]
14) Kodani N, Yamazaki H, Tsubokura T, Shiomi H, Kobayashi K, Nishimura T, et al. Stereotactic body radiation therapy for head and neck tumor: disease control and morbidity outcomes. J Radiat Res 2011;52(1):24-31. [ Özet ]
15) Shah H, Gemmete JJ, Chaudhary N, Pandey AS, Ansari SA. Acute life-threatening hemorrhage in patients with head and neck cancer presenting with carotid blowout syndrome: follow-up results after initial hemostasis with covered-stent placement. AJNR Am J Neuroradiol 2011 Apr;32(4):743-7. [ Özet ]
16) Chang FC, Lirng JF, Luo CB, Guo WY, Teng MM, Tai SK, et al. Carotid blowout syndrome in patients with head-and-neck cancers: reconstructive management by self-expandable stent-grafts. AJNR Am J Neuroradiol 2007 Jan;28(1):181-8. [ Özet ]