


AN UNUSUAL METASTATIC PATTERN OF LARYNX CANCER: THE FOREARM
2Gazi University Faculty of Medicine, Department of Radiation Oncology, Ankara, Turkey
Summary
Early laryngeal cancers usually respond well to treatment, but sometimes the disease may progress aggressively. An adult male patient with T1a glottic cancer underwent narrow field radiation. Initially the disease responded well but in 2 months local recurrence with a tonsillary lesion appeared. The patient underwent a major operation including oropharyngeal resection, total laryngectomy, bilateral neck and paratracheal dissections. Adjuvant chemoradiation was started, but 3 weeks later a biopsy proven metastasis developed on the left forearm. Chemotherapy regimen was readjusted and local radiation was given, but the mass responded partially. Then, lung metastasis developed and the patient died in 3 months.Introduction
Head and neck squamous cell cancer (HNSCC) accounts for 6-10% of all human malignancies, larynx and oropharynx are the most common localizations [1]. Early laryngeal cancers respond well to single modality treatment, but sometimes the disease may progress aggressively despite maximal treatment.HNSCC has a predilection to cervical lymph node metastasis, and hematogenous spread is less frequent. With improved methods of locoregional control, the reported incidence of distant metastasis has risen. It is reported as 3- 8 %, but postmortem studies give figures between 34 and 57% [2-6]. The lung is the most common site involved, followed by mediastinum, bone, central nervous system and other organ systems [2,3]. Unusual metastatic sites such as skin, percutaneous gastrostomy site, small intestines, spleen and scapular muscles are also reported [7].
Metastasis of head and neck carcinoma to the forearm region has not been reported previously to our best knowledge. Uncontrolled progression of a moderately differentiated early cancer of larynx, recurring locally along with a tonsillary cancer is also a rare entity.
Case Presentation
A 56 years old male patient, with a history of heavy smoking (60 pack-year) and regular alcohol consumption (20-30cc/day), presented with hoarseness of 2 months duration. Office examination with mirror and 90 degree rigid endoscopy revealed T1a glottic lesion, limited to right vocal cord and anterior comissure. Computed tomography (CT) scans confirmed endoscopic findings (Figure-I). Neck examination and other physical findings were negative, and blood chemistry was within normal limits.
 Büyütmek İçin Tıklayın |
Figure 1: Computed tomography scan shows T1a glottic lesion, limited to right vocal cord and anterior comissure (arrow). |
Biopsy was performed via direct laryngoscopy under general anesthesia and the findings were consistent with the preoperative assessment. Histopathological examination was reported as moderately differentiated squamous cell cancer. The patient received hyperfractionated 4800 cGy (120 cGy/ fr x2 for 20 days) narrow field radiation to larynx with the diagnosis of stage I glottic carcinoma.
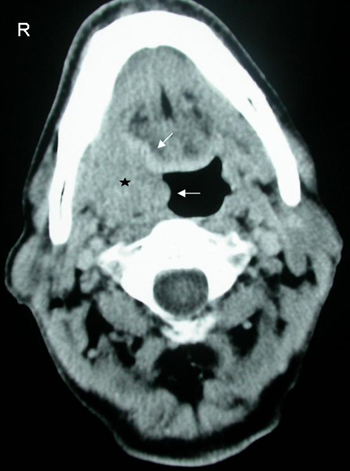
Control office examination 2 months after the completion of radiation revealed minimum edema and thickening of the vocal cords without any lesion. However, within the next 4 weeks the patient developed a right tonsillary mass and hoarseness. On physical examination, there was a 4x3 cm well circumscribed exophytic mass in the right tonsillar fossa and a transglottic lesion involving both cords with subglottic extension and mobile arytenoids. Same lesions (tonsil and larynx) and extralaryngeal extension was detected on CT scans (Figure II, III). The neck was negative as well as the chest CT. Biopsy of both lesions (tonsil and larynx) were reported as squamous cell cancer.
 Büyütmek İçin Tıklayın |
Figure 2: Computed tomography scan shows a 4x3 cm well circumscribed mass (arrows) in the right tonsillar fossa (star). |
 Büyütmek İçin Tıklayın |
Figure 3: Computed tomography scans show a transglottic lesion involving both cords with subglottic (arrow) and extralaryngeal extension (star). |
The patient was diagnosed to have synchronized multiple head and neck cancer, of which one was a radiation failure. He underwent a major surgery including oropharyngeal tumor resection with lip split incision and total laryngectomy, bilateral type III modified radical neck dissection, and paratracheal dissection with modified Conley incisions. Oropharyngeal defect was repaired primarily and so the pharynx. Postoperative period was uneventful, except for minor flap necrosis, and he was discharged on the 10th postoperative day.
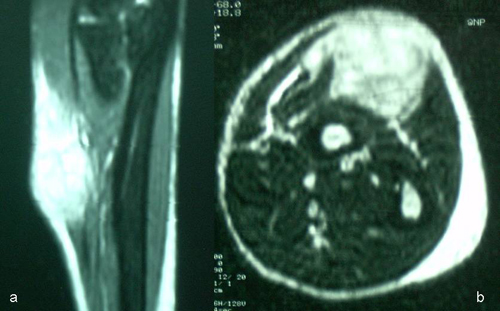
On histopathological examination both specimens were reported as poorly differentiated squamous cell cancer with vascular invasion and negative margins. There was significant subglottic extension and thyroid cartilage invasion. One lymph node was involved at level II on the right site, and 6 nodes were involved bilaterally in the paratracheal region. With these poor prognostic markers adjuvant chemo-radiation was started at the 4th postoperative week. Total dose of 5000 cGy conventional radiation (200 cGy/day) was given to the fields involving bilateral necks, right tonsillary region and upper mediastinum. The chemotherapy included 6 cycles of cisplatin (50mg/m2) given every 3rd week. At the 3rd week of radiation a 3x3 cm subcutaneous swelling appeared on the dorsal aspect of left forearm. The mass enlarged gradually and became fixed in a week. Magnetic resonance imaging (MRI) was obtained which revealed a solid lesion invading the skeletal muscles (Figure IV). CT of the brain and chest was negative for metastasis. Biopsy of this lesion was consistent (squamous cell cancer) with the metastasis of head and neck cancer. The chemotherapy regimen was reorganized and the dose of cisplatin was raised to 100mg/m2 and also taxophene was added. A total dose of 2800 cGy hyperfractionated radiation (200 cGy/fr x2 for 7 days) was given to the forearm with linear accelerator. The forearm lesion was reduced to a size of 2x1 cm and stabilized. However, 2 months later lung metastasis appeared and the patient died after another 3 months.
 Büyütmek İçin Tıklayın |
Figure 4: Sagittal (a) and axial (b) sections of magnetic resonance imaging of the left forearm dorsal region, showing the subcutaneous 4x5 cm solid mass invading the skeletal muscles. |
Discussion
Distant metastasis is the spread of tumor to other organ systems, and can be of two types. First is lymphatic spread to nodes other than regional such as; mediastinal, abdominal or axillary and the second is hematogenous spread [2]. In HNSCC, distant metastasis generally occurs after regional metastasis, and advanced nodal disease increases the incidence by threefold [3].There is no known factor to predict metastasis, but host defense and tumor biology may play role. The explanation to unusual sites of metastasis such as the forearm is even less clear. The disturbance of lymphatic drainage due to surgery and radiation may result in alternative pathways of drainage. This phenomenon can result in lymphatic metastasis of cancer to sites below the clavicle [8]. Another possible explanation is hematogenous spread of the tumor [7].
Our patient with the history of heavy smoking and alcohol initially presented with early laryngeal cancer which recurred shortly after the completion of radiation along with another oropharyngeal lesion. Despite aggressive surgical treatment followed by adjuvant chemo-radiation, the disease metastasized to an unusual distant site. The biological explanation of this tonsillary lesion is a dilemma. Tonsils have no afferent lymphatics, so lymphatic spread from another head and neck primary is a weak possibility. It can be a second primary cancer of oropharynx. Having such an aggressive tumor with unusual metastatic pattern, another possible explanation is the hematogenous spread from the laryngeal primary. Our initial perspective was, the patient had multiple synchronous primary head and neck cancer and we aimed to cure both. However, the pattern of the disease progress seems to be more on the side of an hemotogenous spread.
Such an aggressive behavior manifested by an early laryngeal cancer is a rare entity. In our opinion, unknown factors of host defense and tumor aggressivity may sometimes lead to such situations. However, there is no proven immunological or tumor factor to predict the aggressivity of head and neck cancer.
Reference
1) Sinard RJ, Netterville JL, Garrett CG, Ossoff RH. Cancer of the larynx. In: Myers EN, Suen JY, eds. Cancer of the Head and Neck. Philadelphia (PA): W.B. Saunders Company, 1996: chp 20, 381-421.
2) Spector GJ. Distant metastases from laryngeal and hypopharyngeal cancer. ORL J Otorhinolaryngol Relat Spec 2001; 63:224-228. [ Özet ]
3) Spector JG, Sessions DG, Haughey BH, Chao KS, Simpson J, El Mofty S, Perez CA. Delayed regional metastases, distant metastases, and second primary malignancies in squamous cell carcinomas of the larynx and hypopharynx. Laryngoscope 2001; 111:1079-1087. [ Özet ]
4) Haas I, Hauser U, Ganzer U. The dilemma of follow-up in head and neck cancer patients. Eur Arch Otorhinolaryngol 2001; 258:177-183. [ Özet ]
5) Dennington ML, Carter DR, Meyers AD. Distant metastases in head and neck epidermoid carcinoma. Laryngoscope 1980; 90:196-201. [ Özet ]
6) Bhatia R, Bahadur S. Distant metastasis in malignancies of the head and neck. J Laryngol Otol 1987; 101: 925-928. [ Özet ]
7) Yucel EA, Demirel T, Demiryont M, Egeli U, Deger K. An unusual metastatic site of laryngeal carcinoma: scapular muscles. J Laryngol Otol 2003; 117:85-87. [ Özet ]
8) Alavi S, Namazie A, Sercarz JA, Wang MB, Blackwell KE. Distant lymphatic metastasis from head and neck cancer. Ann Otol Rhinol Laryngol 1999: 108:860-863. [ Özet ]