


REMOVAL OF A GIANT ETHMOIDO-ORBITAL OSTEOMA BY COMBINED ENDONASAL ENDOSCOPIC AND ANTERIOR ORBITAL APPROACH: CASE PRESENTATION
2Şişli Etfal Eğitim ve Araştırma Hastanesi, 1. Göz Hastalıkları Kliniği, İstanbul, Türkiye
Summary
Osteomas are the benign tumors of the paranasal sinuses, mostly seen in the frontal and ethmoid sinuses and less common in the maxillary sinus. A 32- year- old female presented with a 4-year onset of facial asymmetry and a decrease in visual acuity in the left eye, associated with left eye proptosis, periorbital pain, and edema. The purpose of this report is to present a giant osteoma that originating from ethmoid sinus extending to orbit and to discuss the advantages of removal with combined endoscopic endonasal and anterior orbital approach.Introduction
Osteoma which is a benign tumor of the paranasal sinuses is seen mostly in frontal and ethmoid sinuses and less common in the maxillary sinus [1, 2]. Although osteoma is generally asymptomatic, it may be symptomatic in case of intracranial or intraorbital extension. In intraorbital involvement there may be proptosis, diplopia, epiphora, orbital cellulitis, chemosis, amaurosis fugax, orbital emphysema, limitation of eye movement, pain, and decrease in visual acuity [2-6]. We present a case of combined endonasal endoscopic and anterior orbital approach in removal of a giant ethmoidoorbital osteoma which causes a decrease in visual acuity in the left eye, associated with proptosis, periorbital pain, and edema.Case Presentation
A 32- year- old female presented with a 4-year onset of facial asymmetry and left proptosis. The patient had neither a history of head trauma nor paranasal sinuses. She reported a decrease in visual acuity and periorbital pain in left eye at least 2 months. On physical examination, there was an inferolateral left orbital deviation with a slight asymmetry. Left proptosis was evident with lateral displacement of the globe, limitation of eye movement, and periorbital hyperemia. Endoscopic examination of nasal cavity showed normal mucosal appearance and no septal deviation.Axial and coronal computed tomography of the head revealed a 3x3,5 cm centrally hypodense lesion, with well defined margins and bone density, originating from the left ethmoid sinus and extending to the left orbit with destruction of lamina papyrecea. By extending to and destructing the medial orbital wall, the defined mass was displacing the medial rectus muscle laterally and globe anteriorly behind the equator. Left optic nerve was stretched and displaced laterally by mass as well (Fig. 1). Operation was performed by a team of ophtalmologists and otorhinolaryngologists. The mass was exposed after opening the ethmoid bulla and completing left anterior ethmoidectomy endoscopically (Fig. 2). The osteoma could not be removed with a forceps. A diamond drill was used to excise the superior region of the osteoma and to separate from neighboring structures. The mass, which had no connection with ethmoid roof, was mobilized and broken into pieces with a toothed forceps. Then it was decided to excise the portion of the mass causing a defect in lamina papyrecea and extending into the orbit. A curvilinear incision was made medial to inner canthus. Lateral to the lamina papyrecea, soft tissue and periosteum were elevated and the intraorbital portion of the osteoma was exposed. The mass was completely mobilized and removed. Antibiotic- and corticosteroid-soaked sponge was placed between the lamina papyrecea and its periosteum to close the defect. Nasal packing was placed and the external incision was closed. The nasal packing was removed on the 2nd postoperative day. Patient had an uncomplicated post-operative course and was discharged on the 3rd post-operative day. The final pathology report was consistent with eburne (compact) type osteoma. At 2-month follow up, the patient had full range of motion of her left eye but the diplopia, which was initially presented with lateral gaze, was still consistent. At 12-month follow up, the patient was free of diplopia. Recent radiography showed the defect in the lamina papyrecea, but was otherwise normal.
 Büyütmek İçin Tıklayın |
Figure 1: Coronal computed tomography (CT) was showed that large, centrally hypodense mass originated left ethmoid sinus and extending to the left orbit. |
 Büyütmek İçin Tıklayın |
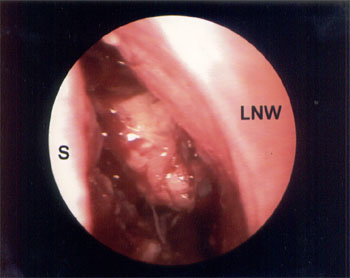
Figure 2: Endoscopic view of the mass after anterior ethmoidectomy. S: (Nasal) septum, LNW: Lateral nasal wall. |
Discussion
Osteomas, the most common benign tumors of the paranasal sinuses, are slow growing and generally asymptomatic tumors and may be diagnosed coincidentally in radiological screening. Osteomas are more frequently found in men than in women. The developmental causation of osteomas is unknown. However, three theories have been postulated for the etiology of osteomas; embryologic, traumatic and infectious [7, 8, 9]. Conheim (cited by Hallberg and Begley) [7] proposed that tumors arise generally at the junctional zone of two tissues of different embryonic origin. The traumatic theory postulated that head trauma might cause excessive bone growth [8]. According to the infectious theory chronic infections stimulate osteoblastic proliferation in mucoperiosteum leading to osseous formation [9]. Osteomas may be one of the manifestations of Gardners syndrome which is characterized by osteomas, intestinal polyposis and multiple dermoid cysts of the skin [5].Histological type of bone formation is either compact osteoma (Ivory-eburneous) which is hard, dense mature bone with small haversian spaces and minimal fibrous tissue; cancellous osteoma (spongiosum) without dense bone, or a mixture of two (osteoma durum) [10].
While surgical intervention is not considered in osteoma which is asymptomatic or does not have intracranial and intraorbital extension, growth rate must be monitorized by periodic radiographs [3, 5]. In follow-up rapid growth is one of the surgical indications [11]. The most common symptom is headache, occurs due to secondary sinus infection and obstruction of the ostium. Hehar and Jones proposed that patients with ethmoid osteoma with persistent headache, regardless of size of osteoma, should be operated after the other reasons of headache have been excluded [12]. While pneumotocele, mucocele, abscess formation, meningitis, and cerebrospinal fluid fistula may be seen in intracranial extension, intraorbital extension causes proptosis, diplopia deviation of globe, limitation of the eye movement, decrease in visual acuity, and far less amaurosis fugax [4, 5, 13].
The traditional approach to small ethmoid osteomas is through a curvilinear medial orbital incision [10]. The transcoronal and through a lateral rhinotomy approach to ethmoid osteomas extending into orbit provide wide exposure for orbital exploration and controlled access to the superior border of the tumor and sinus [5, 10].
The alternative approach to ethmoid osteoma is via the endoscopic route. With its recent advent, endoscopic sinus surgery (ESS) is successfully used in removal of osteoma in paranasal sinuses with the low morbidity, superior cosmetic results, and greater experience [13].
The goal of the surgery is complete removal of the tumor, decompression of the orbital contents and to avoid the damage to the neighboring structures. The combined approach, via endoscopic intranasal and anterior orbital approach, was chosen for our patient. With 0 degree and 30 degree endoscopes could be identified the extent of the tumor and neighboring structures under direct visualization very well. In our patient after ethmoidectomy was identified that the tumor was adhered to the ethmoid roof and was separated with using a drill. The osteoma was then mobilized and was broken into small pieces with a forceps to shrink the tumor which damaged the lamina papyrecea. Through an incision medial to inner canthus the tumor was approached and separated from lacrimal sac and orbital contents. The osteoma was removed through damaged lamina papyrecea without an additional work about surrounding structures.
Although ESS is the procedure of choice in well-selected cases of ethmoid osteoma, combined surgical approaches may be preferred in intraorbital extension of ethmoid osteomas. Combined surgical approach offers a safe and effective alternative with a low morbidity to both open and endoscopic surgery used alone.
Reference
1) Maiuri F, Iaconetta G, Giamundo A, et al.Fronto-ethmoidal and orbital osteomas with intracranial extension. Report of two cases. J Neurosurg Sci 1996;40:65-70 [ Özet ]
2) Goldenberg D, Gilboa M, Danino J, et al. A large ethmoido-orbital osteoma presenting with epiphora in an 11-year-old boy. J Pediatr Ophthalmolog 2000;37:238-40 [ Özet ]
3) Rawe SE, VanGilder JC. Surgical removal of orbital osteoma; case report. J Neurosurg 1976;44:233-36 [ Özet ]
4) Wilkes SR, Trautmann JC, Campbell RJ. Osteoma an unusual cause of amaurosis fugax. Mayo Clin Proc 1979;54:258-260 [ Özet ]
5) Gillman GS, Lampe HB, Allen LH. Orbitoethmoid osteoma: Case report of an uncommon presentation of an uncommon tumor. Otolaryngol Head Neck Surg 1997;117:218-220 [ Özet ]
6) Cecire A, Harrison HC. Ethmoid osteoma, orbital cellulitis and orbital emphysema. Aust NZJ Ophthalmol 1988;16:11-14 [ Özet ]
7) Hallberg OE, Begley JW. Origin and treatment of osteomas of the paranasal sinuses. Arch Otolaryngol 1950;51:750-760.
8) Smith AT. Osseous lesions of nose and sinuses: With special reference to hypertrophic changes and tumor formations. Arch Otolaryngol 1940;31:289-312,.
9) Coates GM, Krauss F. Osteoma of the frontal sinus. Ann Otol Rhinol Laryngol 1941;50:450-457.
10) Marks MW, Newman MH. Transcoronal removal of an atypical orbitoethmoid osteoma. Plast Reconstr Surg 1983;72:874-877 [ Özet ]
11) Barlett JR. Intracranial neurological complications of frontal and ethmoidal osteomas. Brit J Surg 1971;58:607-613 [ Özet ]
12) Hehar SS, Jones NS. Fronto-ethmoid osteoma: The place of surgery. J Laryngol Otol 1997;111:372-375 [ Özet ]
13) Menezes CA, Davidson TM. Endoscopic resection of a sphenoethmoid osteoma: A case report. Ear Nose Throat J 1994;73:598-600 [ Özet ]