


ASSESSMENT OF THE EFFECT OF WIND INSTRUMENTS ON VOICE QUALITY
Summary
Background: In this study, we aimed to perform vocal analysis with objective and subjective parameters in wind instrumentalists and to compare the results with a control group.Methods: The study included 30 musicians who had regularly used a wind instrument for at least 1 year. The control group consisted of 30 healthy subjects who had never played a wind instrument. Subjective and objective voice analyses were performed for both groups.
Results: VHI-10, a subjective parameter, and F0 and HNR, two objective parameters, were higher, and jitter % and shimmer %, which are perturbation parameters, were lower in the study group compared with the control group.
Conclusion: Wind instruments cause changes in the objective and subjective parameters of vocal analysis. Vocal symptoms of the wind instrumentalists were increased, but improvements in the objective parameters of the vocal analyses were detected.
Introduction
Professional wind instrumentalists need to make coordinated use of body structures such as the lungs, vocal tract, oral cavity, and orofacial musculature [1]. The main instruments played by this group of musicians are flute, trombone, saxophone, clarinet, tuba, oboe, bassoon, cornet, trumpet, French horn, and euphonium. Players can play quite long passages, up to perhaps 50 seconds in duration, without requiring to take a breath, with the throat and mouth filled with air from the lungs under high pressure to maintain the instrument"s sound [2]. It necessitates heavy use of the neck muscles, pulmonary function, and diaphragmatic support in longer musical notes [3,4].During the execution of playing wind instruments, the expired air exerts pressure on the vocal tract, and the pharynx constricts and relaxes. Mukai emphasized that the glottis controls air flow by contracting while using these instruments [5]. Contraction of the glottis while making sound causes strain and discomfort in the larynx and eventually laryngeal lesions may occur. Dysphonia, an increase in secretion, interarytenoid edema, hyperemia, vocal polyps, gastroesophageal reflux symptoms, and laryngopharyngeal diverticula due to excessive pressure in the pharynx can be seen in wind instrumentalists [3,6-8].
Although there are studies about changes in the larynx due to playing wind instruments resulting in symptoms, we found no publications about changes in objective voice parameters in this musician group in the literature. In this study, we aimed to perform vocal analysis using objective and subjective parameters in wind instrumentalists and to compare the results with a control group.
Methods
Study populationThe present study was conducted at XXXX City Hospital in the otolaryngology outpatient clinic with 60 volunteers. We planned to include 30 musicians who had regularly used a wind instrument for at least 1 year in the study group. In this group, there were 3 trumpet players, 5 trombone players, 8 saxophone players, 4 tuba players, 4 baritone players, and 6 clarinet players. The control group consisted of 30 healthy subjects who had never played a wind instrument. The age of the volunteers was between 18 and 53 years, and for standardization, all selected volunteers were men. The oral cavity and nasal cavity, nasopharynx, and larynx were examined in all participants. Volunteers with a history of infection, septum deviation, allergic rhinitis, reflux laryngitis, asthma, oropharynx, and nasopharynx lesions were excluded from the study. Those with a history of laryngeal intubation within the last 3 months, and especially with a laryngeal pathology (e.g., polyp, nodule, and Reinke edema), were also excluded from the study.
Subjective and objective voice analyses were performed for both groups
Subjective voice analysis
The Turkish version of the Voice Handicap Index 10 (VHI-10) scale was used to evaluate the vocal symptoms of the participants, which were evaluated between 0 and 4. The scores increase as the vocal symptoms increase [9]. The VHI-10 results were compared between the groups.
Objective voice analysis
The Paul Boersma and David Weenink voice analysis system (Praat) is one of the leading voice analysis programs. All participants were seated in a quiet room, and analysis was performed from voice samples collected through a 20-cm high-quality dynamic microphone (Audio Technica at 2020) connected to a computer. Voice samples were elicited by asking each participant to produce sustained phonations of the /a/ sound at their habitual levels of pitch and loudness. The investigator ensured that each participant was comfortable and competent in producing sustained phonations at their habitual levels. Three sustained phonations (with each phonation lasting longer than 3 seconds) were then recorded. The second production was used for data analysis. To rule out the effects of onset and offset voicing, the segment analyzed was a 1-s portion in the middle of the vowel production. The selected segments were later digitized (50-kHz sampling rate) and analyzed using Praat, and we chose five Praat acoustic parameters of voice. The other Praat parameters were excluded as irrelevant for the experiment"s purposes. The fundamental frequency F0, jitter %, shimmer %, and harmonics-to-noise ratio (HNR) were measured on acoustic voice analysis. F0, jitter %, shimmer %, HNR values, and VHI-10 were statistically compared between the two groups.
Statistical analysis
The normality of the data was checked using the Shapiro-Wilk test. Parametric and non-parametric tests were performed according to the normality condition of the data. Student's t- test was used to compare mean ages between the study and control groups, and the Mann-Whitney U test was used to compare median values of mean pitch F0, shimmer %, jitter %, HNR dB, and VHI-10 parameters.
The data were analyzed using the IBM Statistical Package for the Social Sciences (SPSS) Version 22.0 package program (Armonk, NY). The significance value of 0.05 was used to interpret the results; P < 0.05 was considered statistically significant.
Results
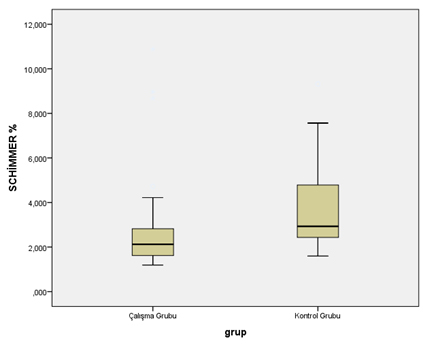
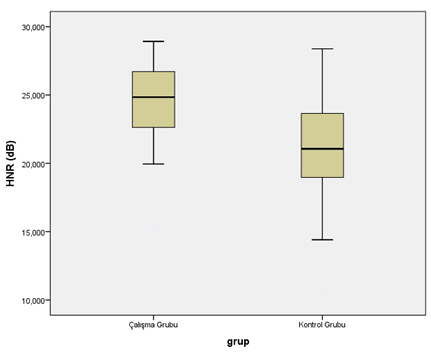
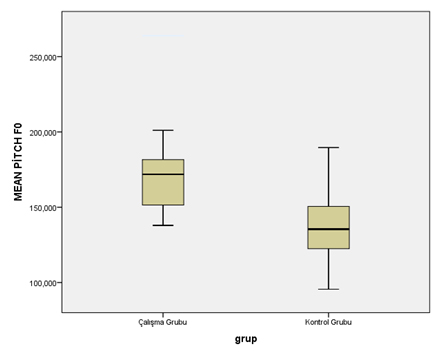
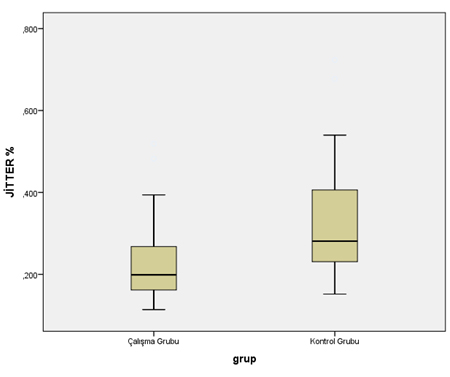
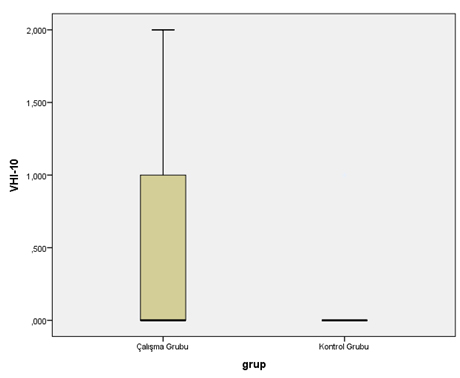
There were statistically significant differences between the study and control groups in terms of medians of all parameters in the acoustic analyses. VHI-10, a subjective parameter, and F0 and HNR, two objective parameters, were higher, and jitter % and shimmer %, which are perturbation parameters, were lower in the study group compared with the control group (Table 1) (Figure 1-5).){kind=link}
Table 1: Comparison of objective and subjective acoustic parameters
 Büyütmek İçin Tıklayın |
Figure 1: Comparison of shimmer % between the groups. |
 Büyütmek İçin Tıklayın |
Figure 2: Comparison of HNR dB between the groups. |
 Büyütmek İçin Tıklayın |
Figure 3: Comparison of mean pitch FO between the groups |
 Büyütmek İçin Tıklayın |
Figure 4: Comparison of jitter between the groups. |
 Büyütmek İçin Tıklayın |
Figure 5: Comparison of VHI-10 between the groups. |
There was no statistically significant difference between the different wind instruments in terms of VHI-10, F0, jitter %, shimmer %, and HNR averages in the study group (Table 2-6).
){kind=link}
){kind=link}
Table 2: Comparison of wind instruments according to jitter values
Table 3: Comparison of wind instruments according to F0 values
){kind=link}
Table 4: Comparison of wind instruments according to shimmer values
){kind=link}
Table 5: Comparison of wind instruments according to HNR db value
){kind=link}
Table 6: Comparison of wind instruments according to VHI-10 values
Discussion
The aim of the present study was to evaluate the effects of wind instruments on vocal parameters and to compare these results with those of a control group. We found an increase in VHI-10, a subjective parameter, an increase in F0 and HNR, two objective parameters, and a decrease in jitter and shimmer in musicians who played wind instruments.In previous studies, the importance of vocal cords was emphasized in the formation of musical notes [3,10]. The changes caused by wind instruments in the larynx were investigated. The main symptoms that can occur in wind instrumentalists include dry throat, irritability, pain, and cervical muscle pain. The production of sound in wind instrumentalists requires high effort, which can cause dehydration in the oral cavity and larynx, leading to changes in the voice [1,11]. A study investigated whether the voice was affected in patients with dry mouth through objective parameters and it was found to be affected negatively [12].
There are many wind instruments such as trumpet, trombone, saxophone, tuba, baritone, and clarinet, and the playing technique of each differs from the others. The techniques of playing the instruments affect the physiology of the aerodigestive tract. There is high tension in the lips and the muscles on the face while playing any of these instruments [13]. Playing them requires coordination of the respiratory tract, effective airway, robust diaphragmatic support, appropriate mucociliary function, and humidification. Neck, chest, and abdominal muscles also support the diaphragm. In this way, there are changes in the air column depending on the instrument used over time. Musicians using a wind instrument produce sound with precise manipulations of air flow. A disturbance or discoordination in the maintenance of air flow will lead to inefficient sound production [3].
In the subjective evaluation of the voice, many different scales have been used in the literature. In a study of vocal tract diseases in wind instrumentalists, the Voice-Related Quality of Life (V-RQOL) scale was used and according to the results, social-emotional subscores, functional subscores, and total subscores were found to be in parallel with the vocal tract discomfort scale score [1]. We used the Turkish version of VHI-10 in our study, which is a simplified questionnaire used in the subjective evaluation of voice analysis, and may be used as a guide in the early detection of voice diseases. In our study, this value was found to be significantly higher in the group that played instruments.
Objective vocal analysis is a non-invasive, easy-to-perform test that may be comfortably used to monitor the effects of diseases on the voice. F0, jitter %, shimmer %, and HNR measurements in voice analysis are important and adequate for identifying the acoustic characteristics of voice. F0 would be sensitive to structural and physiological changes in the vocal folds tension and increase in HNR in periodic portions of speech was said to reflect a more efficient function of vocal fold vibration [14,15]. In our study, both F0 and HNR values were significantly higher in the wind instrumentalist group. Jitter and shimmer are the two common perturbation measurements in acoustic analysis. These two measurements are used to verify the perturbation level in the voice signal, and they are modestly correlated with voice quality characteristics such as hoarseness or roughness [16]. In our study, jitter and simmer values were significantly lower than the control group. The lower perturbation measures and higher HNR and F0 in wind instrumentalist group compared to control group indicate better control of phonatory and respiratory system resulting in improved voice quality because of long-term using instrument habits.
According to the results of acoustic vocal analysis in studies performed in professional singers, differences in F0 and decrease jitter value were observed [17,18]. In other studies performed on musicians, the increase in F0 was specifically highlighted [19,20]. These changes were linked to increased lung capacity and better vocal control in occupational groups who required more pressure to project their voices [20]. All these studies were performed in professional singers who used their voices excessively, showing that objective parameters were changed. We thought that the objective parameters could change in wind instrumentalists in the same way so we planned to perform this study. Our results are in line with the results of those studies performed in singers. We found that F0 was significantly higher and jitter and shimmer were significantly lower in wind instrumentalists compared with the study group.
The first limitation of our study is that it was performed in a limited number of volunteers. Similar studies with more individuals performed in the future will contribute to the literature. Second, it would be useful to monitor whether the voices of individuals in the study group changed over time and to repeat the same tests in the same individuals at different time points, but we did not provide a follow-up in the volunteers because of the cross-sectional nature of our study.
Reference
1) Cappellaro J, Beber BC. Vocal Tract Discomfort and Voice-Related Quality of Life in Wind Instrumentalists. J Voice. 2018 May;32(3):314-18. [ Özet ]
2) Fletcher NH. The physiological demands of wind instrument performance. Acustics Australia 2000; 28: 53-6
3) Gallivan G, Eitinier C. Vocal fold polyp in a professional brass/wind instrumentalist and singer. J Voice. 2006;20:157-64. [ Özet ]
4) Weikert M, Their J. Laryngeal movements in saxophone playing: video-endoscopic investigations with saxophone player. J Voice. 1999; 13:265-73. [ Özet ]
5) Mukai S. Laryngeal movements during wind instrument play. Nippon Jibiinkoka Gakkai Kaiho. 1989;92:260-70. [ Özet ]
6) Eckley CA. Glottic configuration in wind instrument players. Rev Bras Otorrinolaringol. 2006;72:45-7. [ Özet ]
7) Cammarota G, Masala G, Cianci R, et al. Reflux symptoms in wind instrument players. Aliment Pharmacol Ther. 2010;31:593-600 [ Özet ]
8) Costa MM1, Alvite FL. Lateral laryngopharyngeal diverticula: a videofluoroscopic study of laryngopharyngeal wall in wind instrumentalists. Arq Gastroenterol. 2012 Apr-Jun;49(2):99-106. [ Özet ]
9) Reliability and validity of the Turkish version of the Voice Handicap Index. Kiliç MA, Okur E, Yildirim I, Oğüt F, Denizoğlu I, Kizilay A, Oğuz H, Kandoğan T, Doğan M, Akdoğan O, Bekiroğlu N, Oztarakçi H.
Kulak Burun Bogaz Ihtis Derg. 2008 May-Jun;18(3):139-47. [ Özet ]
10) Chapman RR. A strategy for proper utilization of the glottis and implications of improper use in trumpet performance. Open Access Dissertations. Paper 1188; 2014.
11) Sivasankar M, Fisher KV. Oral breathing increases Pth and vocal effort by superficial drying of vocal fold mucosa. J Voice. 2002;16:172-81. [ Özet ]
12) Roh JL, Kim HS, Kim AY. The effect of acute xerostomia on vocal function. Arch Otolaryngol Head Neck Surg. 2006;132:542-6. [ Özet ]
13) Ocker C, Pasher W, Ro¨hrs M, Katny W. Voice disorders among players of wind instruments? Folia Phoniatr. 1990;42:24-30. [ Özet ]
14) Colton, R. H., Casper, J. K., & Leonard, R. (2011). Understanding voice problems: A physiological perspective for diagnosis and treatment (4th ed.). Philadelphia: Lippincott Williams and Wilkins
15) Van Lancker Sidtis D, Rogers T, Godier V, Tagliati M, Sidtis JJ. Voice and fluency changes as a function of speech task and deep brain stimulation. J Speech Lang Hear Res. 2010;53:1167-1177.
16) Natour YS, Darawsheh WB, Bashiti S, et al. A study of VHI scores and acoustic features in street vendors as occupational voice users. J Commun Disord. 2018;71:11-21 [ Özet ]
17) Brown WS, Rothman HB, Sapienza CM. Perceptual and acoustic study of professionally trained versus untrained voices. J Voice. 2000;14:301-9. [ Özet ]
18) Mendes AP, Rothman HB, Sapienza C, et al. Effects of vocal training on the acoustic parameters of the singing voice. J Voice. 2003;17:529-43. [ Özet ]
19) Preethi R. Comparison of Dysphonia Severity Index (DSI) in trained carnatic classical singers and non-singers India: University of Mysore; 2013.
20) Acoustic and Aerodynamic Characteristics of Choral Singers. Ravi SK, Shabnam S, George KS, Saraswathi T.J Voice. 2018 Jul 10. [ Özet ]