


THE SIGNIFICANCE OF HISTOPATHOLOGIC TONSILLAR ACTINOMYCOSIS IN PEDIATRIC PATIENTS WITH RECURRENT ACUTE TONSILLITIS
2Süleyman Demirel University Faculty of Medicine, Department of Patology, Isparta, Turkey
Summary
Background: The aim of this study is to determine the possible role of Actinomyces histopathologically found in tonsillar tissue on hypertrophy, fibrosis, and asymmetry of tonsils in patients with recurrent acute tonsillitis.Materials and Methods: One hundred and fifty consecutive patients underwent tonsillectomy with the diagnosis of recurrent acute tonsillitis were enrolled in this study. Tonsillectomy specimens stained with haematoxylin-eosin were all evaluated with light microscopy for the presence of Actinomyces. Patients with tonsillar specimens showing Actinomyces were involved in the study group and those without any findings of Actinomyces were involved in the control group. Two groups of patients were compared with respect to the concomitant adenoid hyperplasia, season of operation, age, gender, duration of disease, the degree of tonsillar hypertrophy and tonsillar asymmetry and fibrosis. Data were analyzed by SPSS statistics package. The Chi-squared and ANOVA tests were performed.
Results: One hundred and fifty consecutive patients with a mean age of 8.38 ± 3.74 years (ranging from 3 to 16) were enrolled in this study. Actinomyces were determined in 53 (35,3 %) patients. Patients operated on during summer season, and having longer periods of complaints before surgery, female gender and older mean age had significantly more frequent Actinomyces in their tonsillar tissues (chi-square test: P <.05). The other parameters were not different between two groups.
Conclusions: In contrary to some other studies the presence of Actinomyces in tonsillar tissue is an incidental finding. It is the colonization of tonsils by Actinomyces which does not have any clinical importance.
Introduction
Actinomyces are anaerobic, gram positive, non-acid fast, branched, filamentous bacteria. They colonize in gingival crypts, dental calculi and tonsillar crypts.[1,2] The presence of Actinomyces in tonsils is not synonymous with clinical fulminant disease, although it is mostly referred as tonsillar actinomycosis.[1] The relationship between actinomycosis and adenotonsillar disease has been investigated in some studies. However, results were not consistent because of methodology of these studies.[1,3] The aim of this study was to investigate possible role of Actinomyces found in histopathologic section of tonsillar tissue of patients with the diagnosis of recurrent acute tonsillitis (RAT).Methods
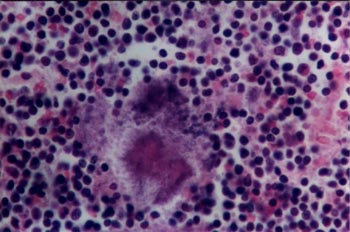
One hundred and fifty consecutive patients underwent tonsillectomy with the diagnosis of RAT were enrolled in this prospective study. Patients with the diagnosis of other than RAT such as; chronic adenotonsillar hypertrophy without a history of RAT, peritonsillar abscess, known craniofacial anomaly, suspicion of tumor were not included in this study. The indications of tonsillectomy due to RAT were according to one of the following criteria; 1) Seven or more acute tonsillitis attacks in the preceding year, 2) Five or more acute tonsillitis attacks in the 2 preceding years, 3) Three or more acute tonsillitis attacks in the (at least) 3 preceding years.4 All the patients were operated on under general anesthesia. The operation technique was dissection following cold knife incision. During operation tonsillar measurements were obtained in order to get hypertrophy grading for each tonsil. The size of each tonsil was recorded according to classification of Brodsky et al.,[5]: Grade 0; Tonsils are entirely within the tonsillar fossa. Grade 1; Tonsils occupy less than 25 % of the lateral dimension of the oropharynx as measured between anterior tonsillar pillars at mid-tonsil level. Grade 2; Tonsils occupy 25-50 % of the lateral dimension of the oropharynx as measured between anterior tonsillar pillars at mid-tonsil level. Grade 3; Tonsils occupy 50-75 % of the lateral dimension of the oropharynx as measured between anterior tonsillar pillars at mid-tonsil level. Grade 4; Tonsils occupy more than 75 % of the lateral dimension of the oropharynx as measured between anterior tonsillar pillars at mid-tonsil level. Concomitant adenoid hyperplasia, season of operation, age, gender, duration of disease, the degree of tonsillar hypertrophy and tonsillar fibrosis were all recorded.All surgically removed tonsils were fixed in formalin, embedded in paraffin and finally prepared serial microscopic slides were stained with haematoxylin-eosin. All microscopic slides were evaluated under light microscopy (Nikon Optiphod-B) by two pathologists unfamiliar with clinical findings of patients other than surgical diagnosis of RAT. Actinomycosis was recognized as aggregates of filamentous basophilic microorganisms arranged in a radial spoke-like fashion (Figure 1).[6] Patients with tonsillar specimens containing actinomycotic focus or foci were included in study group, and patients with no focus of actinomycosis were included in control group. Both tonsils of the same patient were evaluated separately when comparing the fibrosis within the tissue and hypertrophy grading scale of tonsils. However, both tonsils of the same patient were evaluated as one in case of comparison of parameters such as concomitant adenoid hyperplasia, season of operation, age, gender, duration of disease. Comparison between study and control group was based on these criteria. Data were recorded in Microsoft Excel database. All analyses were performed using SPSS 10.0 for Windows (SPSS., Chicago, IL). Chi-squared test was applied to find out the statistical significance of the association between various factors and the presence of the actinomycosis. One-way ANOVA and spearman’s rank-order correlation were used for analysis of tonsillar hypertrophy grading between two groups. P values less than .05 was accepted as significant.
 Büyütmek İçin Tıklayın |
Figure 1: Histopathologic section of tonsil demonstrating a radial spoke like fashion appaerance of a tonsillar actinomycosis (haematoxylin-eosin, original magnification 200 X). |
Results
One hundred and fifty consecutive patients were undergone to tonsillectomy with the diagnosis of RAT. Of the 150 patients with RAT, 79 were male and 71 were female. Patients’ age were between 3 and 16 years (mean age was 8.38 ± 3.74 years). Fifty three (35.3 %) patients with actinomycosis in their tonsillar tissue were included in study group and 97 patients (64.7 %) without actinomycosis in their tonsillar tissue specimens were included in control group. The mean age of study group patients (9.33 ± 3.16) was significantly older from those of control group (7.85 ± 3.94) (p = .004). Of the 53 patients with actinomycosis, 24 were male and 29 were female. Of the 97 patients without actinomycosis, 55 were male and 42 were female. There is statistically significant gender difference between two groups (p = .03). Patients operated on during summer session and with longer duration of complaints have had higher incidence of actinomycosis in their tonsillar tissue than others (p = .03, p = .001). There were 23 patients with tonsillar asymmetry; 9 from actinomycosis group and 14 from control group (p = .33). There was no significant difference between two groups regarding concomitant adenoid hyperplasia, tonsillar hypertrophy grading, tonsillar asymmetry and fibrosis of tonsillar tissue (Table. 1, 2).){kind=link}
){kind=link}
Table 1: Patients demographics and several factors between two groups.
Table 2: Evaluation of each tonsillar actinomycosis regarding tonsillar hypertrophy and fibrosis.
Discussion
Actinomycosis is a well-known infection reported in several anatomic locations of body, such as; oral cavity, pharynx, maxilla, mandible, temporal mandibular joint, neck, mediastinum, thyroid gland, salivary gland, middle ear and central nervus system.[2,7] The ability to identify actinomycosis histologically is straightforward and has a higher yield than culture. Although culture is classically believed to be the most definitive means of identification, there are a high number of false negative results reported. This may be due to culture overgrowth by other organisms, failure of growth following antibiotic therapy and failure of growth due to inadequate anaerobic conditions.[6] Since the biopsy of infected tissues, including tonsils, has been shown to be diagnostic we have preferred to search tonsillar actinomycosis histopathologically instead of culturing.The frequency of tonsillar actinomycosis was reported to be as high as 56 % in the literature. [1] The reason of great differences in frequency among several studies may be contributed to staining technique, indications for surgery and regional differences.[3] Our study indicates that the Actinomyces in tonsillar tissue is a colonization; this may also explain the great differences in tonsillar actinomycosis incidence. Women are infected much less frequently than are men.[2] On the other hand, Gaffney et al.,[3] have found no gender preponderance of the tonsillar actinomycosis in patients with RAT. Their study group was patients with RAT and control group was patients with the diagnosis other than tonsillitis. Age range was very different between two groups (2-34 years in study group and 27-80 years in control group). There was a female preponderance of tonsillar actinomycosis in our study. This may be explained by methodology of the study, environmental, cultural factors and/or women may be more susceptible to infection. Regional differences and environmental risk factors for colonization of tonsils with actinomycosis would also explain this difference. A correlation between actinomycosis and tonsillar hypertrophy has been proposed in a study conducted by Bhargawa et al.[1] Whereas, the indications for tonsillectomy were different in these studies.[1,6] We have compared hypertrophy grading of tonsils in patients with the same surgical indications. Thus, the misleading effects of different surgical indications were eliminated in this study. We found no effect of actinomycosis on the tonsillar hypertrophy grading. High frequency of actinomycosis in patients operated on during summer session may be explained by colonization of oral cavity during this period of year. Harley[8] found no statistically significant difference between patients with asymmetric and symmetric tonsils regarding to the presence of actinomycosis in tonsillar tissue. We had 23 patients with tonsillar asymmetry; 9 from actinomycosis group and 14 from control group. Our finding was correlated with that of Harley.[8]
During the course of actinomycosis infection there is a characteristic woody type of fibrosis and suppuration.[2] In our study, however, there was no statistically significant difference between two groups with respect to tonsillar fibrosis. This also favors that; tonsillar actinomycosis is a colonization of tonsils, not a disease process affecting the clinical course.
Reference
1) Bhargava, D., Bhusnurmath, B., Sundaram, KR., Raman R, Al Okbi HM, Al Abri R, Date A. 2001. Tonsillar actinomycosis: a clinicopathological study. Acta Tropica 80, 163-168. [ Özet ]
2) Richtsmeier, WJ., Johns, ME. Actinomycosis of the head and neck. 1979. CRC Crit Rev Clin Lab Sc. 11, 175-202. [ Özet ]
3) Gaffney, R., Harrison, M., Walsh, M., Sweeney, E., Cafferkey, M. 1993. The incidence and role of actinomyces in recurrent acute tonsillitis. Clin Otolaryngol 18, 268-271. [ Özet ]
4) Wiatrak, BJ., Woolley, AL. Pharyngitis and adenotonsillar disease. In: Cummings, CW., Frederickson, JM., Harker, LA., Krause, CJ., Richardson, MA., Schuller, DE (Es.), Otolaryngology Head Neck Surgery, vol. Pediatric, third ed., pp. St. Louis, Mosby, 1998:202-204..
5) Brodsky, L., Moore, L., Stanievich JF. 1987. A comparison of tonsillar size and oropharyngeal dimensions in children with obstructive adenotonsillar hypertrophy. Int J Pediatr Otorhinolaryngol 13, 149-156. [ Özet ]
6) Pransky, SM., Feldman, JI., Kearns, DB., Seid, AB., Billman, GF. 1991. Actinomycosis in obstructive tonsillar hypertrophy and recurrent tonsillitis. Arch Otolaryngol Head Neck Surg 117, 883-885. [ Özet ]
7) Olson, TS., Seid, AB., Pransky, SM. 1989. Actinomycosis of the middle ear. Int J Pediatr Otorhinolaryngol 17, 51-55. [ Özet ]
8) Harley EH. 2002. Asymmetric tonsil size in children. Arch Otolaryngol Head Neck Surg 128, 767-769. [ Özet ]