


EVALUATION OF NOISE INDUCED HEARING LOSS IN AIRPORT GROUND HANDLING WORKERS
2İstanbul Medipol Üniversitesi, Sağlık Bilimleri Fakültesi, Odyoloji Bölümü, İstanbul, Turkey
3Turkish Do&Co Airline Catering, İstanbul, Turkey
Summary
Objective: This study aims to evaluate the hearing loss of airline staff working in different departments according to the noise level they are exposed to and to draw attention to the importance of protection from the negative effects of noise.Materials and Methods: 512 airline staff working in different departments were included in the study. The noise levels in the departments were determined and grouped. The pure tone audiometry test for job entry and the most recent pure tone audiometry test of the staff participating in the study were scanned. The results were evaluated according to the department and the noise level.
Results: As a result of the evaluation, a statistically significant difference was found in all frequencies of the preparation and delivery staff, (Group 1) (p<0.05). While there was no significant difference in the right ear of 0,25 kHz and 1 kHz in the left ear of the dishwashing staff (Group 2), a statistically significant difference was found in the other frequencies (p<0.05). While there was no significant difference at 0,25, 1, 2 kHz in the right ear and 2 kHz in the left ear of the cleaning staff, (Group 3), a statistically significant difference was found in other frequencies (p<0.05).
Conclusion: It is thought that not using/not using ear protectors correctly for employees exposed to noise cannot provide an effective level of protection. In addition, those working in noisy environments should receive training on how to protect themselves from noise by an expert and different protection/intervention strategies should be applied.
Introduction
Occupational hearing loss as a result of exposure to noise is an important health problem worldwide[1]. Noise-induced hearing loss (NIHL) has been reported as the second most common cause of acquired hearing loss after presbycusis, with occupational noise exposure accounting for 16% of cases that cause hearing loss[2,3].Hearing loss can lead to communication difficulties, social isolation, stress, and fatigue if precautions are not taken. In addition, hearing loss is associated with increased health problems, such as depression, cognitive decline, and dementia[4,5].
NIHL is a sensorineural type of hearing loss that is typically bilateral, notching at 3, 4, or 6 kHz affecting high frequencies but showing some improvement at 8 kHz[6]. The duration, intensity, and frequency of the noise, as well as the person's age, genetics, and physiological factors, all play a role in the degree, type, and configuration of hearing loss[7].
Loud noise damages the auditory system by affecting the hair cells and auditory nerve cells in the cochlea[8]. Permanent hearing loss occurs as a result of sudden or continuous noise exposure. One of the working environments that cause noise is the airport. It has been reported that there is a very high noise level especially in the ground handling department[9].
In this study, the noise level and hearing test results of airport ground handling workers exposed to occupational noise were evaluated according to their departments, and the effect of noise on hearing thresholds was examined. At the same time, in this study, it was aimed to draw attention to the necessity of protection from the negative effects of noise on hearing health.
Methods
This study was conducted in a catering company. Prior to the study, approval was obtained from the Ethics Committee (24.12.2020/958).A total of 512 staff members (393 males and 119 females) between the ages of 20 and 56 (38.58 ± 6.79) were included in the study. The pure tone audiometry test (PTAT) results of airline staff members were analyzed retrospectively. Persons who worked less than 1 year and had a single audiogram were not included in the study. The employment PTAT and recent PTAT results of the included individuals were evaluated. Air conduction (AC) of 0.25-8 kHz was scanned for both ears.
Participants were grouped according to the departments they worked in. Noise measurements were measured with a sound level meter. The noise levels were determined by measuring the noise in the departments where they worked.
Group 1: 95-140 dB(A)/ Preparation and delivery staff,
Group 2: 85-100 dB(A)/ Cleaning staff,
Group 3: 85-100 dB(A)/ Dishwashing staff
Statistical analysis of the data was performed with IBM SPSS Statistics (25.0). The conformity of the data to the normal distribution was evaluated by visual (histogram and scatter plots) and statistical (Kolmogorov Smirnov-Shapiro Wilks) methods. Since the frequency comparison of the scanned hearing tests did not show a normal distribution, the Wilcoxon T-test was applied. The statistical significance level was accepted as p ≤ 0.05.
Results
Table 1 shows the descriptive statistics regarding the demographic characteristics of the staff.){kind=link}
Table 1: Demographic Information
According to the pure tone average of the staff evaluated at the beginning of the job, 487 staff members had normal hearing in the right ear; this number decreased to 458 in the most recent evaluation. The number of people with mild hearing loss increased to 48, the number of people with moderate hearing loss increased to 4, and the number of people with moderate to severe hearing loss increased to 2. The number of staff members with normal hearing in the left ear decreased from 488 to 461 in the last evaluation. The number of people with mild hearing loss increased to 42, and the number of people with severe hearing loss increased to 2 (Table 2).
){kind=link}
Table 2: Hearing Loss Degrees of Staff
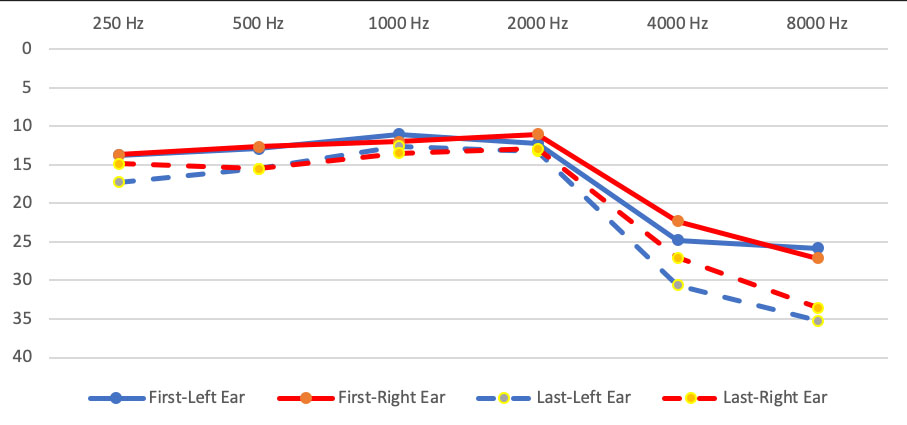
In the Wilcoxon T analysis performed to compare the AC thresholds in the first and last tests, a statistically significant difference was obtained in all frequencies, bilaterally, in Group 1. (Right: p=0,000; p=0,000; p=0,000; p=0,044; p=0,000; p=0,000) (Left: p=0,049; p=0,000; p=0,001; p=0,000; p=0,000; p=0,000) (Table 3).
){kind=link}
Table 3: Right and Left Ear Air Conduction Results of Staff
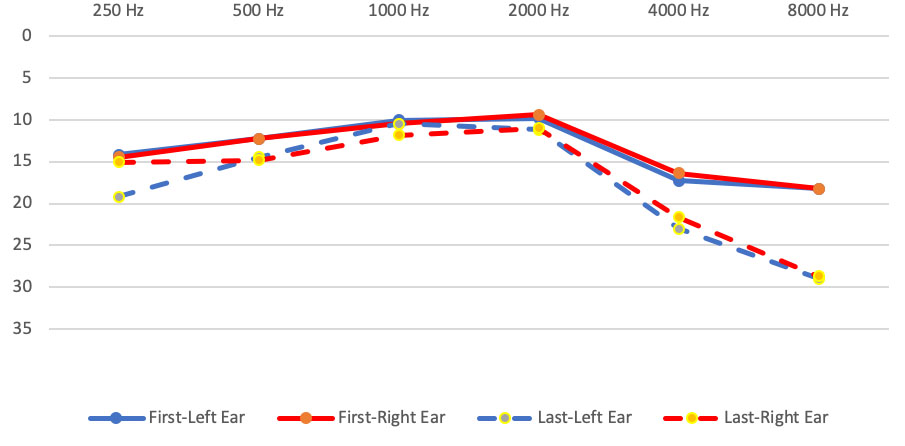
For staff members in Group 2, a statistically significant difference was found between the thresholds of the right ear at 0.5, 1, 2, 4, and 8 kHz and the left ear at 0.25, 0.5, 2, 4, and 8 kHz at the entrance to work and the last hearing test thresholds (Right: p=0,000; p=0,001; p=0,000; p=0,000; p=0,000) (Left: p=0,000; p=0,000; p=0,001; p=0,000; p=0,000). In this group, no statistically significant difference was found in the comparison of 0.25 kHz in the right ear and 1 kHz in the left ear Right: p=0,456) (Left: p=0,475) (Table 3).
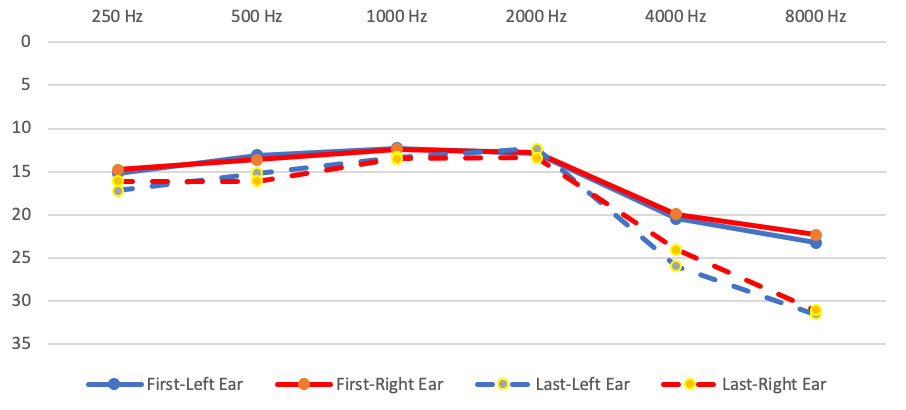
In Group 3, a statistically significant difference was found between the thresholds of the right ear at 0.5, 4, and 8 kHz and the left ear at 0.25, 0.5, 4, and 8 kHz at the beginning of the job and the last hearing test thresholds (Right: p=0,015; p=0,000; p=0,000) (Left: p=0,034; p=0,023; p=0,002; p=0,000; p=0,000). There was no significant difference in the right ear at 0,25, 1, 2 kHz and left ear at 2 kHz in this group (Right: p=0,299; p=0,197; p=0,722) (Left: p=0,482) (Table 3).
The 0.25-8 kHz AC threshold average of the first PTAT performed by Group 1 staff members before they entered the job and the PTAT they had after they were employed are presented in Figure 1.
 Büyütmek İçin Tıklayın |
Figure 1: Hearing Threshold Average of Group 1 (dB HL) |
The 0.25-8 kHz AC threshold average of the first PTAT performed by Group 2 staff members before they entered the job and the PTAT they had after they were employed are presented in Figure 2.
 Büyütmek İçin Tıklayın |
Figure 2: Hearing Threshold Average of Group 2 (dB HL) |
The 0.25-8 kHz AC threshold average of the first PTAT performed by Group 3 staff members before they entered the job and the PTAT they had after they were employed are presented in Figure 3.
 Büyütmek İçin Tıklayın |
Figure 3: Hearing Threshold Average of Group 3 (dB HL) |
Discussion
NIHL is one of the most common and preventable causes of occupational morbidity[10]. It has many serious consequences, including limitation of communication, that can significantly affect social integration, functional ability, self-esteem, work performance, and quality of life outside of work. Considering its significant impact on people's lives and society, NIHL is becoming a major concern for health professionals[11,12].If there is a different degree of noise exposure between the two ears in NIHL, there may be some asymmetrical consequences of hearing loss. In the literature, it is seen that NIHL tends to be more severe in the left ear; approximately 90% of the world's population is right-handed, and some have suggested that right-handed people turn their left ear toward the noise source[11,12,13]. This result is consistent with the findings of our study, in which it was observed that the left ear was more affected at 4 and 8 kHz in all groups (Table 3).
Nair et al. (2009), in their study with 1,000 staff members in the Indian Air Force, demonstrated that the significant difference in the prevalence of NIHL is due to the fact that the departments are exposed to different noise levels[14]. Also, Novastuti et al. (2019) states in his study that hearing loss is mostly in the preparation and delivery department[9]. This situation supports our research and it was observed that Group 1 had the highest increase in hearing loss (Table 3).
Suter (2002) pointed out that both low and high frequencies will be affected whenever there is long-term exposure to loud noise without appropriate protection[15]. In our study, it was observed that Groups 1, 2, and 3 were all affected at low frequencies (Table 3).
Anino et al. (2010) found in their study that there were different effects on various units at the airport. It has been determined that cargo and freight staff are also exposed to excessive aircraft noise on the cargo ramp[16]. In addition, group 1 is constantly exposed to noise from ground equipment such as tractors, trucks, conveyor belts, and trolleys. The cargo terminal and aircraft ramp have previously been shown to have excessive noise levels[17].
Nasir and Rampal (2012) studied hearing loss and contributing factors in a study of 358 staff at Malaysia Airport. In the study, a significant difference was also obtained in cases such as the duration of exposure to noise and smoking[18]. The retrospective nature of our study led to limitations in examining some factors.
Literature review among airport ground handling staff has showed that there is no study related to hearing loss especially in cleaning and dishwashing staff. This indicates a gap in the current scientific literature on the subject. This being the first study conducted on cleaning and dishwashing staff, we hope it will lead to future studies.
If occupational diseases are not monitored, they can progress without being diagnosed[19]. For this reason, it is important to monitor the hearing of employees with periodic check-ups for early diagnosis and prevention of NIHL through a hearing protection program[20]. In addition to periodic controls, changes in the work program of the staff, training the staff and employers will be an effective way to eliminate or reduce industrial noise[11-21]. In addition, it has been observed in NIHL that personalized hearing protectors are effective in preventing noise[22]. It has been reported that these protectors cannot provide an effective level of protection unless the workers are instructed on their proper use[23].
Conclusion
In this study, it was revealed that exposure of airline personnel to noise affects hearing test results. For this reason, for the promotion of personalized hearing protection products, it is necessary for those working in noisy environments to receive training on this subject and for audiologists to apply different intervention strategies for hearing.It will contribute to industrial audiology if NIHL summarizes the situation in our country by conducting projects and scientific studies with more researchers.
Financial Support: This research received no grant from any funding agency/sector.
Conflicts of Interest: The authors declared that there is no conflict of interest.
Reference
1) Nelson DI, Nelson RY, Concha-Barrientos M, Fingerhut M. The global burden of occupational noise-induced hearing loss. Am J Ind Med. 2005;48(6):446-458. doi:10.1002/ajim.20223 [ Özet ]
2) Vos T, Flaxman AD, Naghavi M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010 (published correction appears in Lancet. 2013 Feb 23;381(9867):628. AlMazroa, Mohammad A (added); Memish, Ziad A (added)). Lancet. 2012;380(9859):2163-2196. doi:10.1016/S0140-6736(12)61729-2 [ Özet ]
3) Imam L, Hannan SA. Noise-induced hearing loss: a modern epidemic?. Br J Hosp Med (Lond). 2017;78(5):286-290. doi:10.12968/hmed.2017.78.5.286 [ Özet ]
4) Basner M, Babisch W, Davis A, Brink M, Clark C, Janssen S, Stansfeld S. Auditory and non-auditory effects of noise on health. Lancet. 2014;383(9925):1325-1332. doi:10.1016/S0140-6736(13)61613-X [ Özet ]
5) Themann C, Suter AH, Stephenson MR. National Research Agenda for the Prevention of Occupational Hearing Loss-Part 1. Semin Hear 2013; 34(03): 145-207.
doi:10.1055/s-0033-1349351
6) Mirza R, Kirchner DB, Dobie RA, Crawford J; ACOEM Task Force on Occupational Hearing Loss. Occupational Noise-Induced Hearing Loss. J Occup Environ Med. 2018;60(9):e498-e501. doi:10.1097/JOM.0000000000001423 [ Özet ]
7) Zeren S, Bolulu A, Köse B, Ocak S, Topal A, Kurt E, Barut AY. Üniversite Öğrencileri ve Çağrı Merkezi Çalışanlarının İşitme Sağlığı Bilgisi ve İşitme Kaybı Farkındalığı. IGUSABDER. 2018; (6): 573-584.
8) Özgüven, H. N. Gürültü Kontrolü. Ankara: Türk Akustik Derneği Yayını, 35-196; 2008.
9) Novastuti CD, Purnami N, Affianti N. Noise Induced Hearing Loss in Ground Handling Workers at Juanda Airport Surabaya. Korean J Otorhinolaryngol-Head Neck Surg 2020; 63(2): 59-63. doi:https://doi.org/10.3342/kjorl-hns.2019.00353
10) Le TN, Straatman LV, Lea J, Westerberg B. Current insights in noise-induced hearing loss: a literature review of the underlying mechanism, pathophysiology, asymmetry, and management options. J Otolaryngol Head Neck Surg. 2017;46(1):41. Published 2017 May 23. doi:10.1186/s40463-017-0219-x [ Özet ]
11) Hong O, Kerr MJ, Poling GL, Dhar S. Understanding and preventing noise-induced hearing loss. Dis Mon. 2013;59(4):110-118. doi:10.1016/j.disamonth.2013.01.002 [ Özet ]
12) Sayler SK, Roberts BJ, Manning MA, Sun K, Neitzel RL. Patterns and trends in OSHA occupational noise exposure measurements from 1979 to 2013. Occup Environ Med. 2019;76(2):118-124. doi:10.1136/oemed-2018-105041 [ Özet ]
13) Dement J, Welch LS, Ringen K, Cranford K, Quinn P. Hearing loss among older construction workers: Updated analyses. Am J Ind Med. 2018;61(4):326-335. doi:10.1002/ajim.22827 [ Özet ]
14) Nair S, Kashyap RC. Prevalence of Noise Induced Hearing Loss in Indian Air Force Personnel. Med J Armed Forces India. 2009;65(3):247-251. doi:10.1016/S0377-1237(09)80015-4 [ Özet ]
15) Suter A. Hearing Conservation Manual. 4th ed. Milwaukee: CAOHC; 2002.
16) Anino JO, Afullo A, Otieno F. Occupational noise-induced hearing loss among workers at Jomo Kenyatta International Airport, Nairobi. East Afr Med J. 2010;87(2):49-57. doi:10.4314/eamj.v87i2.60599 [ Özet ]
17) Mutinda, D. Kenya Airways Noise Level Survey Report. Kenya Airways, Nairobi. 2004.
18) Nasir HM, Rampal KG. Hearing loss and contributing factors among airport workers in Malaysia. Med J Malaysia. 2012;67(1):81-86. [ Özet ]
19) Hearing Conservation. (Washington, D.C.?): U.S. Dept. of Labor, Occupational Safety and Health Administration; 2002.
20) Caldart A, Adriano C, Igor Terruel I, Martins R, Mocellin M. The prevalence of noise
induced hearing loss among textile industry workers. Int Arch Otorhinolaryngol 2006;
10:10-14. doi: 10.4103/1012-5574.138484
21) Rabinowitz PM, Galusha D, Kirsche SR, Cullen MR, Slade MD, Dixon-Ernst C. Effect of daily noise exposure monitoring on annual rates of hearing loss in industrial workers. Occup Environ Med. 2011;68(6):414-418. doi:10.1136/oem.2010.055905 [ Özet ]
22) Sriwattanatamma P, Breysse P. Comparison of NIOSH noise criteria and OSHA hearing conservation criteria. Am J Ind Med. 2000;37(4):334-338. doi:10.1002/(sici)1097-0274(200004)37:4<334::aid-ajim2>3.0.co;2-z [ Özet ]
23) Kerr MJ, Neitzel RL, Hong O, Sataloff RT. Historical review of efforts to reduce noise-induced hearing loss in the United States. Am J Ind Med. 2017;60(6):569-577. doi:10.1002/ajim.22627 [ Özet ]