


COMPARISON OF COMPUTED TOMOGRAPHY, MAGNETİC RESONANCE IMAGING AND POSITRON EMISSION TOMOGRAPHY IN DETECTING CARTILAGE INVASION IN LARYNX CANCERS
2Recep Tayyip Erdogan University Faculty of Medicine, Radiology, Rize, Turkey
3Muğla Sıtkı Koçman University Faculty of Medicine, Nuclear Medicine, Mugla, Turkey
4Imperial Hospital, Otorhinolaryngology, Trabzon, Turkey
5Recep Tayyip Erdogan University Faculty of Medicine, Pathology, Rize, Turkey
6Altunbaş University Faculty of Medicine, Otorhinolaryngology, Istanbul, Turkey
7Lokman Hekim University Faculty of Medicine, Otorhinolaryngology, Ankara, Turkey
Summary
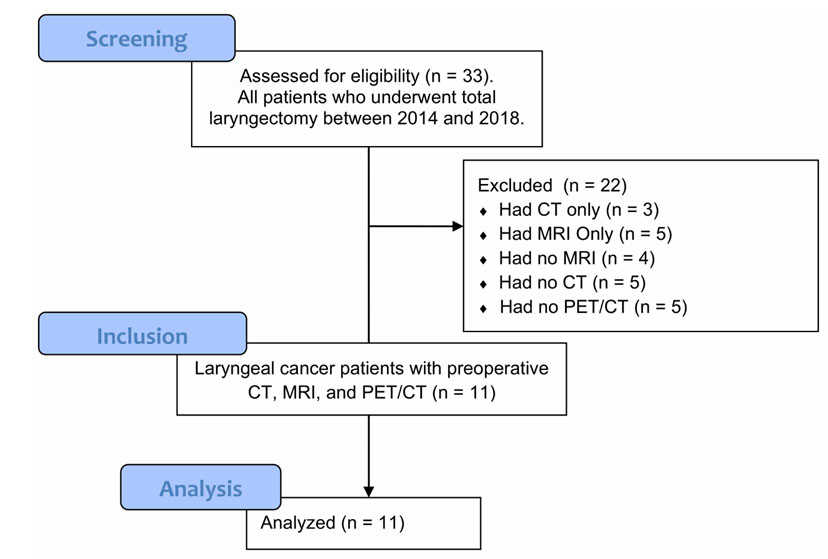
Objective: Laryngeal cancer is the most common malignancy of the head and neck region, following skin tumors. Cartilage invasion is an important feature in staging of laryngeal cancers. This study compared three frequently used radiologic tests used to detect cartilage invasion in laryngeal cancers.Materials and Methods: Medical records of 33 patients, who underwent total laryngectomy between 2014 and 2018, were retrospectively reviewed. Data from 11 patients, who had undergone both PET/CT, CT, and MRI were analyzed. The radiologic test results were re-evaluated for cartilage invasion by one radiologist and one nuclear medicine specialist experienced in head and neck cancers, who were blinded to any other patient data. The scores given by the examiners were compared with the pathology specimen results to form a confusion matrix.
Results: All except 1 patient were male (91%). The mean age was 64 years (51-80). All except 1 patient had a history of smoking. TNM staging was T4a in 6 patients, T2 in 4 patients, and T3 in 1 patient. Two patients received salvage surgery after radiotherapy. Most frequent tumor localization was transglottic. PET/CT, CT, and MRI methods were all 83.3% sensitive, specificity was 80%, 60%, 40%; positive predictive value was 83.3%, 75%, 62.5%; negative predictive value was 72.7%, 66%, 80%, and the accuracy was 81.8%, 72.7%, 63.6%, respectively.
Conclusions: Despite similar sensitivity, PET/CT examination scored best in specificity, positive and negative predictive value, whereas MRI scored worst.
Introduction
Laryngeal cancers are the second most common cancer of the head and neck region[1]. It is more prevalent in men: 5.7 in every 100,000 person vs 0.4 in women. The incidence of any form of laryngeal cancer in Turkish men is 2.2%, which makes it the10th most prevalent tumor in men[2].Staging is the most important part in the treatment plan. While a single treatment modality is chosen in early-stage laryngeal cancers, multi-modality treatments should be applied in advanced-stage. Thyroid cartilage invasion is one of the important features to distinguish early and advanced stage laryngeal cancers. Also, it is long known that the efficacy of radiotherapy is low in patients with cartilage invasion[3]. Therefore, detection of thyroid cartilage invasion in laryngeal cancers is of utmost importance in the treatment plan. Both CT and MRI are used to detect cartilage invasion. The detection rate depends on the experience of the radiologist, thus these two imaging modalities are used interchangably or together.
PET/CT is recommended in patients with advanced stage. These patients have already undergone either CT or MRI. This study aimed to compare the diagnostic rate of cartilage invasion in the three imaging modalities. Fort his purpose, a retrospective study was designed to compare the results of the imaging modalities and histopathologic results.
Methods
Following approval of the Ethics Committee for Non-invasive Studies (decision no: 2023/25), medical records of patients, who underwent total laryngectomy between 2014 and 2018, in Recep Tayyip Erdogan University Training and Research Hospital, Department of Otorhinolaryngology. Patients who had preoperative CT, MRI and PET/CT examinations were included in the study. The imaging examinations were re-evaluated for cartilage invasion by one radiologist and one nuclear medicine specialist, experienced in head and neck cancers and blinded tot other patient data. The evaluation results were compared with the results of histopathological examinations to form confusion matrices. The data were analyzed with Excel (Office 365, 2022).Results
Data from a total of 11 patients were analyzed. STROBE diagram was given in Figure 1, and patient characteristics were given in Table 1.){kind=link}
 Büyütmek İçin Tıklayın |
Figure 1: STROBE diagram of the study. |
Table 1: Patient characteristics.
Briefly, all except one patient were male. The single female patient was the only non-smoker and had a tumor stage of T4a. The two patients who had a salvage surgery after radiotherapy had tumor stages of T3 and T4a.
The results obtained from the confusion matrix was given in Table 2. Briefly, all imaging modalities showed the same sensitivity. PET/CT scored best in the rest of the parameters, whereas MRI scored worst.
){kind=link}
In detail, PET/CT was able to correctly identify 9 out of 11 patients, and 8 out of 9 patients who received no radiotherapy. Patients with low-grade tumour had no cartilage invasion in pathological specimens. CT and PET/CT showed 1 false positive, each. MRI showed 2 false positives, one of which was due to false positive sclerosis. Six out of seven patients with high-grade tumors had cartilage invasion. CT showed 1 false positive and 1 false negative. PET/CT and MRI showed 1 false negative, each.
Table 2: Sensitivity, specificity, predictivity and accuracies of the imaging modalities.
Discussion
This study with a very limited sample size showed that all imaging modalities were equally sensitive. PET/CT had the highest specificity, predictive value and accuracy. In contrast with the current literature, MRI had the worst scores.To our knowledge, there are few studies comparing the PET/CT with conventional imaging in laryngeal cancer. However, only one of these studies compared cartilage invasion with conventional imaging methods. In that study, Paone et al. evaluated radiological imaging findings of 27 patients. All patients had cartilage invasion. They reported that MRI was 100% sensitive and specific, whereas PET/CT was 95% sensitive and CT was 70% sensitive. The specificity of PET/CT and CT was found as 86%[4].
PET/CT has gained an important place in the staging of head and neck cancers in recent years. PET/CT provides not only anatomical information, but also functional information[5]. The role of PET/CT in the assessment of cartilage invasion is unclear. Kats et al. determined the relationship between tumor size and cartilage invasion in patients who were not treated with radiotherapy. It has been reported that considering tumor size can be a useful method in estimating cartilage invasion. However, previous studies have reported that CT has limitations in demonstrating cartilage invasion in patients who have received radiotherapy[6]. In another study, although PET/CT was not helpful in patients who did not receive radiotherapy; It is considered as a method that can be used to detect cartilage invasion in patients who have received radiotherapy treatment[7]. In our study, PET/CT stands out as the most valuable method in demonstrating cartilage invasion. These advanced stage patients, also represent our target group from another point of view as they include the group with cartilage invasion in staging. Another limitation of the current study is that CT and MRI images were not made with a superficial coil for the larynx. In addition, the difference in the time between the imaging methods and surgery is another limitation.
Albano et al. examined the detection rates of nodal metastases by comparing imaging methods with each other. The number of patients in whom all three imaging methods were performed together is observed as 10 in this study[8]. Despite the small sample size of our study, we encounter similar numbers when the literature is examined.
Detection of cartilage invasion before treatment in patients with laryngeal cancer was an important point because of its low response to radiotherapy treatment and its association with high local recurrence, where complications caused by radiotherapy especially increased the risk of radionecrosis[9]. Cartilage invasion in laryngeal carcinomas directly causes the disease to be T3 or T4[10]. Detection of thyroid cartilage invasion is of great importance since surgical treatment of advanced laryngeal carcinomas is preferred over the early stages of treatment modalities[11]. There are studies reporting that CT is not effective in detecting cartilage invasion in early stage laryngeal cancers and anterior commissure lesions[12]. Studies have reported that diffusion-weighted MRI is highly reliable in excluding cartilage invasion due to its high sensitivity and negative predictive values, but the specificity and positive predictive values are not satisfactory[13,14]. Many authors recommend MRI as the first choice in the evaluation of cartilage invasion[11,14,15].
Diagnostic criteria for cartilage invasion on computed tomography include sclerosis, lysis, erosion, and extralaryngeal invasion. The most prominent diagnostic criterion is extralaryngeal spread, and the least specific is sclerosis[3]. It is known in studies that sclerosis has a low predictive value in detecting cartilage invasion in laryngeal malignancies[12]. It has been reported that the rate of thyroid cartilage sclerosis on CT in predicting pathological thyroid cartilage invasion in advanced laryngeal carcinomas is as low as 15%[16]. False positive detection of cartilage invasion by preoperative imaging methods leads to overtreatment, and false negative detection leads to low local control[16,17]. Although low local control (42%) was achieved with radiotherapy in tumors adjacent to the thyroid cartilage, this rate was found to be higher (95%) in tumors that were not adjacent to the thyroid cartilage[18]. However, it is thought that thyroid cartilage inner cortex involvement does not pose any risk in terms of local control in patients undergoing surgery[12].
Age-related, sometimes asymmetrical ossifications of the thyroid cartilage can be confused with areas of lysis and erosion; when sclerosis is difficult to distinguish from normal ossification. In addition, even without thyroid cartilage invasion, an increase in osteoblastic activity can be observed in the thyroid cartilage due to the presence of tumor[3]. It has been shown that microscopic invasions of the thyroid cartilage can be missed by computed tomography[19].
Magnetic resonance imaging (MRI) has a higher positive predictive value than CT, and this rate varies between 93 and 96%[20,21]. Contrast enhancement at the level of thyroid cartilage in contrast-enhanced MRI suggests cartilage invasion. Due to the nonspecific properties of MRI, this rate drops to 55%, and this brings many false positives[3,21]. In addition, MRI should be carefully applied and evaluated because it is affected by respiration and motion artifacts[3].
Studies have found a good correlation between CT and MRI in low-grade laryngeal carcinomas. By combining the data of MRI and CT images, higher accuracy results can be obtained in early stage tumors[21]. In a study, it was determined that PET/CT had a high specificity in patients who underwent total laryngectomy. In the same study, CT and MRI tended to exaggerate the size and extent of the gross tumor mass relative to PET/CT and pathology. However, all three imaging methods failed to show superficial mucosal extensions[21]. Recently, it has been reported that intense heterogeneous deposition on the thyroid cartilage in bone scintigraphy predicts thyroid cartilage invasion to a high degree[22].
In conclusion, PET/CT can be used in addition to CT and MRI in detecting cartilage invasion in laryngeal cancers. Studies with larger and homogeneous groups are needed for clearer and more reliable data.
Acknowledgments: We would like to express our gratitude to Associate Professor Dr. Başar Erdivanlı for his valuable contributions and insightful comments that greatly aided us in the preparation of this article.
Reference
1) DeSantis C, Naishadham D, Jemal A. Cancer statistics for African Americans, 2013. CA: a cancer journal for clinicians. 2013;63(3):151-66. [ Özet ]
2) Sağlık Bakanlığı Sağlık İstatistikleri Yıllığı. 2020. p. p. 40-2. .
3) Becker M. Neoplastic invasion of laryngeal cartilage: radiologic diagnosis and therapeutic implications. European journal of radiology. 2000;33(3):216-29. [ Özet ]
4) Paone G, Martucci F, Espeli V, Ceriani L, Treglia G, Ruberto T, et al. (18)F-FDG-PET/CT Imaging in Advanced Glottic Cancer: A Tool for Clinical Decision in Comparison with Conventional Imaging. Contrast Media Mol Imaging. 2019;2019:4051206. [ Özet ]
5) Park G, Kim J, Roh J-L, Choi S-H, Nam S, Kim S. Prognostic value of metabolic tumor volume measured by 18F-FDG PET/CT in advanced-stage squamous cell carcinoma of the larynx and hypopharynx. Annals of oncology. 2012;24(1):208-14. [ Özet ]
6) Kats SS, Muller S, Aiken A, Hudgins PA, Wadsworth JT, Shin DM, et al. Laryngeal tumor volume as a predictor for thyroid cartilage penetration. Head & neck. 2013;35(3):426-30. [ Özet ]
7) Kendi AT, Corey A, Magliocca KR, Galt JR, Zhang C, Chen Z, et al. Is there a role for PET/CT parameters to differentiate thyroid cartilage invasion from penetration? Eur J Radiol. 2016;85(2):319-23. [ Özet ]
8) Albano D, Dondi F, Paderno A, Nocivelli G, Maddalo M, Magrini SM, et al. 18F-FDG-PET/CT in laryngeal cancer: comparison with conventional imaging and prognostic role. Rev Esp Med Nucl Imagen Mol (Engl Ed). 2021;40(4):229-38. [ Özet ]
9) Zbären P, Becker M, Läng H. Staging of laryngeal cancer: endoscopy, computed tomography and magnetic resonance versus histopathology. European archives of oto-rhino-laryngology. 1997;254(1):S117-S22. [ Özet ]
10) Amin MB, Greene FL, Edge SB, Compton CC, Gershenwald JE, Brookland RK, et al. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population?based to a more "personalized" approach to cancer staging. CA: a cancer journal for clinicians. 2017;67(2):93-9. [ Özet ]
11) Castelijns JA, Becker M, Hermans R. Impact of cartilage invasion on treatment and prognosis of laryngeal cancer. European radiology. 1996;6(2):156-69. [ Özet ]
12) Hartl DM, Landry G, Bidault F, Hans S, Julieron M, Mamelle G, et al. CT-scan prediction of thyroid cartilage invasion for early laryngeal squamous cell carcinoma. European Archives of Oto-Rhino-Laryngology. 2013;270(1):287-91. [ Özet ]
13) Becker M, Zbären P, Laeng H, Stoupis C, Porcellini B, Vock P. Neoplastic invasion of the laryngeal cartilage: comparison of MR imaging and CT with histopathologic correlation. Radiology. 1995;194(3):661-9. [ Özet ]
14) Taha MS, Hassan O, Amir M, Taha T, Riad MA. Diffusion-weighted MRI in diagnosing thyroid cartilage invasion in laryngeal carcinoma. European Archives of Oto-Rhino-Laryngology. 2014;271(9):2511-6. [ Özet ]
15) Zbären P, Becker M, Läng H. Pretherapeutic staging of laryngeal carcinoma: clinical findings, computed tomography, and magnetic resonance imaging compared with histopathology. Cancer: Interdisciplinary International Journal of the American Cancer Society. 1996;77(7):1263-73. [ Özet ]
16) Beitler JJ, Muller S, Grist WJ, Corey A, Klein AM, Johns MM, et al. Prognostic accuracy of computed tomography findings for patients with laryngeal cancer undergoing laryngectomy. Journal of clinical oncology. 2010;28(14):2318-22. [ Özet ]
17) Li B, Bobinski M, Gandour-Edwards R, Farwell DG, Chen A. Overstaging of cartilage invasion by multidetector CT scan for laryngeal cancer and its potential effect on the use of organ preservation with chemoradiation. The British journal of radiology. 2011;84(997):64-9. [ Özet ]
18) Murakami R, Furusawa M, Baba Y, Nishimura R, Katsura F, Eura M, et al. Dynamic helical CT of T1 and T2 glottic carcinomas: predictive value for local control with radiation therapy. American journal of neuroradiology. 2000;21(7):1320-6. [ Özet ]
19) Kazkayasi M, Önder T, Özkaptan Y, Can C, Pabuscu Y. Comparison of preoperative computed tomographic findings with postoperative histopathological findings in laryngeal cancers. European archives of oto-rhino-laryngology. 1995;252(6):325-31. [ Özet ]
20) Connor S. Laryngeal cancer: how does the radiologist help? Cancer imaging. 2007;7(1):93. [ Özet ]
21) Daisne J-F, Duprez T, Weynand B, Lonneux M, Hamoir M, Reychler H, et al. Tumor volume in pharyngolaryngeal squamous cell carcinoma: comparison at CT, MR imaging, and FDG PET and validation with surgical specimen. Radiology. 2004;233(1):93-100. [ Özet ]
22) Kurooka H, Kawabe J, Tsumoto C, Hayashi T, Oe A, Kotani J, et al. Examination of pattern of RI accumulation in thyroid cartilage on bone scintigraphy. Annals of nuclear medicine. 2009;23(1):43-8. [ Özet ]