


THE EFFECT OF THE FREQUENCY MODULATION (FM) ASSISTIVE LISTENING DEVICE ON SCHOOL PERFORMANCE IN FIRST GRADE PRIMARY SCHOOL STUDENTS WITH COCHLEAR IMPLANTS: A LONGITUDINAL STUDY
2Department of Otorhinolaryngology, Unit of Hearing Speech and Balance, Dokuz Eylul University, Izmir, Turkey
3Faculty of Education, Division of Measurement and Evaluation in Education, Ege University, Izmir, Turkey
4Faculty of Medicine, Department of Otorhinolaryngology, Unit of Hearing Speech and Balance, Dokuz Eylul University, Izmir, Turkey
5Faculty of Medicine, Department of Otorhinolaryngology, Dokuz Eylul University, Izmir, Turkey
Summary
Aim: Acoustic problems can have untoward effects on academic performance especially in children with hearing loss. This study aimed to determine whether frequency modulation (FM) assistive listening device affects school performance in first grade primary school students with cochlear implants (CIs).Materials and Methods: Ten children were included in the CI group and 10 children were included in the CI + FM (frequency modulation) group. The CI group did not use any hearing assistive devices, whereas the CI + FM group used the FM system regularly. A total of three children from the two groups were excluded from the study for different reasons as of the second measurement. Achievement tests were developed to assess the school performance and fundamental skills acquired via Turkish, mathematics, and life sciences subjects. The tests were administered to the students in both groups at baseline and in three-month intervals, making a total of four measurements.
Results: The results showed a significant increase in students' performance (p< 0.05) in both groups throughout the study. Compared to the CI group, the students in the CI + FM group improved their performance statistically more in mathematics and Turkish achievement tests (p< 0.05).
Conclusions: The study results suggest that the use of the FM system contributes significantly to the school performance of children with CI.
Introduction
For the majority of children with normal learning potential who have undergone early cochlear implants (CIs), the option of formal education in the same classroom with their peers is recommended by experts[1-3]. Although the inclusion of children with CIs in formal education reduces their educational expenditure and increases their academic development, social cohesion, and communication skills[4], it brings about some problems in the classroom. Reverberation effect, background noise, and distance from the sound resource (teacher's voice) impair speech perception[5]. Such acoustic problems can harm students' academic achievement and performance, as they can have a detrimental effect on students' ability to distinguish and understand speech[6]. Especially for children with hearing problems[7] or learning difficulties[8], poor classroom acoustics may have a negative impact.The benefits of the early use of CI in children, especially in language skills development, are known. Most children with CIs before the age of two were found to have similar verbal language skills with their normal-hearing peers[9,10]. Some studies have also found that children implanted before three and attending mainstream schools obtained similar scores with normal-hearing (NH) children[11,12]. Early CI contributed to language development, academic achievement, and regular school attendance similar to their peers with NH[13]. However, CI has limited ability to improve speech perception due to room acoustic problems[5]. Studies have found that speech perception performance of individuals with CI in a noisy environment is 40% lower than in a quiet environment[14-16].
The American National Standards Institute (ANSI) recommends the appropriate acoustic environment for every student in an educational setting. ANSI's 'American National Standard Acoustical Performance Criteria, Design Requirements, and Guidelines for Schools' has been adopted as national classroom acoustics standards. Accordingly, the noise level should not exceed 35 dBA in an empty classroom. It has also been suggested that the reverberation time of an ideal classroom should be less than 0.6 seconds for small classrooms (10,000 sft) and less than 0.7 seconds for large classrooms[17]. The signal to noise ratio (S/N) in the classroom environment should be at least +15 dB. In a typical classroom setting, S/N varies between +1 and +3 dB. Therefore, while reaching a +15 dB S/N without raising the teacher's voice in a typical classroom environment is not sufficient even for a child with normal hearing, at least a + 25- + 30 dB S/N is required for children with hearing loss[18]. Therefore, when the ideal S/N is not reached for children to fully understand speech, the negative effect of poor classroom acoustics on children's auditory performance, which comprises 75% of a school day, is better understood[19].
The use of assistive listening devices (ALDs) is offered as a solution to minimize acoustic problems in the classroom environment for students with hearing aids (HAs) or cochlear implants (CIs), allowing the signal to reach the child directly without distortion. Personal frequency modulation (FM) systems, as a type of ALD, are devices that increase the signal-to-noise ratio (S/N) by transmitting the signal amplified by FM radio waves directly from the transmitter microphone placed on the speaker to the receiver on the listener[20]. In this sense, the FM system is considered one of the most effective technological resources to remedy such difficulties, contributing to improvements in speech perception[21]. Therefore, the difficulty perceiving speech in typical noisy classroom conditions encourages the use of signal-to-noise enhancing technology for children using HAs or CIs[5].
Choi et al. found that most implanted children had more problems in school in a noisy background than at home[22]. Half of the implanted children were found to have difficulty in understanding the teacher. In this study, it was suggested that personal FM systems could provide a better listening environment to improve classroom performance for children with CI and poor speech perception. Many studies have reported that these ALDs improve sound quality, ease of listening, speech recognition in noise, and intelligibility for children with hearing technology[5,23]. Studies have reported that when children use these technologies, these systems improve sound quality, ease of listening, speech recognition in noise, and intelligibility[5,23]. Anderson et al. asked school-age children who used HAs or CIs from an early age to repeat their HINT sentence lists in a condition with typical background noise and echo time. In three different experimental settings, students used a classroom sound field system, a desktop personal sound field FM system, and a personal FM system, respectively, besides amplification devices. When using the personal FM system and desktop personal sound field FM system, their correct reading rate was higher. Besides, most of the participants stated that the personal FM system made it easier to listen[24]. A meta-analysis study also supports that personal FM systems provide more benefits in recognizing speech in noise for children with hearing loss than other type of FM systems[25]. However, students with hearing loss who used personal FM systems were more successful than those who did not. Families, teachers, and students have reported the benefit of FM system at school and home environments[18,26].
This study aimed to examine the effect of personal FM system on school performance of primary school first-grade students with CI as assessed via achievement tests during one academic year. This is a significant research considering the limited number of studies in the literature regarding the contribution of the FM system in the school environment.
Methods
ParticipantsThe study included children who volunteered to participate in the study, who were 6-8 years old, who had severe bilateral sensorineural hearing loss, who had a unilateral cochlear implant for at least three years, who attended a special education and rehabilitation center or kindergarten/nursery regularly after CI surgery, who did not have a disability other than hearing loss, who had their regular CI control for adjustments, and who did not have any transportation issues to attend the study visits at scheduled times for the tests and controls.
G-Power 3.1 (Universitat Dusseldorf, Germany) statistical program was used to determine the sample size[27]. When the literature was examined, a significant difference with an effect size (Cohen's d) of 1.78 was found in the effect of using a personal FM system in the classroom environment on the academic domain of children with auditory processing disorder and healthy controls with normal hearing[28]. In our study, it was predicted that a similar level of difference would be found between the academic success of the CI and CI+FM groups. Therefore, it was calculated that 10 participants should be included in each group to detect this difference with 95% power and 5% type 1 error rate.
Out of 30 children with CI screened for the study, 20 were found suitable to be included in the study. The participants were divided into two groups as the "CI+FM" group (n=10), including participants using both the FM system and CI and the "CI" group (n=10), including participants using only CI.
The follow-up files of pediatric patients, who underwent cochlear implantation surgery, were reviewed to select the children meeting the inclusion criteria. Preliminary information about the study was provided to the families of the children via phone calls. General information was obtained from the families, including the date of birth of the child, the date of the CI operation, the status of attending special education and rehabilitation programs, and the place of residence. Based on the information obtained, volunteering families and children were invited to the clinic to select eligible volunteers to recruit. The Denver II developmental screening test was administered to all the eligible volunteers to detect a developmental disability other than hearing loss in children.
In addition to the Denver-II Developmental Screening Test, the Turkish Expressive and Receptive Language Test (TIFALDI) and the Metropolitan School Maturity Test were administered to the participants in our clinic during the group assignment process.
We calculated the z-scores for each of the three tests using the participants" scores for each test. We took the average of the total z-scores obtained from the three tests to have the overall z-score. We calculated the inter-percentile range using the overall z-score. Participants were ranked by the inter-percentile ranges from low to high values. Participants with a similar or the same inter-percentile range and using the same CI brand were matched. When one of the matched participants was randomly included in the CI + FM group, the other participant was placed in the CI group. Thus, we ensured the formation of equivalent groups regarding the language development, overall development, and school readiness. Furthermore, gaps between individual differences that could affect the assessment results during the year were minimized. In other words, assigning participants according to their matching characteristics ensured the equivalence of the groups.
Participants were evaluated in their schools for all assessments after the groups were formed. One participant in the CI group and two participants in the CI + FM group were excluded from the study as of the second assessment due to transportation problems and loss of FM system devices. The study was completed with 17 students: 8 children in the CI + FM group and 9 in the CI group. Children from 16 different schools and 4 cities participated in the study. Each participating child had nearly 30 peers in the classroom. Similar curricula and similar auditory-verbal training styles were delivered to the participants. Demographic information of the participants is shown in Table 1.
){kind=link}
The mean age was 81±5.09 months for the CI + FM system group and 78±5.51 months for the CI group. The mean age of hearing loss diagnosis was 13±8.32 months for the CI + FM system group and 8±4.84 months for the CI group. Cochlear implantation age mean was 31±9.04 months for the CI + FM system group and 25±7.03 months for the CI group. Duration of CI use was 49±8.92 months for the CI + FM system group and 53±7.82 months for the CI group. Special education duration was 67±6.56 months for the CI + FM system group and 70±8.55 months for the CI group. None of the participants had any contralateral HA use after CI. All except two participants in both groups had prelingual onset of deafness.
According to MannWhitney U test, there were no significant differences between the two groups regarding demographics.
Table 1: Demographic information of participants
After obtaining approval from the Local Ethics Committee (Protocol No: 15-1.1/15), the study was conducted in compliance with the Declaration of Helsinki. Verbal and written informed consent was obtained from all participants and their parents.
Equipment
FM system device
The Phonak MLxi Dynamic FM system and the Zoomlink + Dynamic FM system were used as FM system receivers and transmitters, respectively.
The families and teachers of the participants in the CI + FM group were informed about the use of the FM system. Then, a demonstration was performed for hands-on practice. The families and teachers were provided with guidelines on the use of the FM system. The participants used the FM system regularly during school hours and in the classroom for approximately 8 hours a day.
Seating arrangements were set in cooperation with respective teachers of the participants in the CI group. All students in the CI and CI + FM groups were seated in a standardized seating order in the front row to remain directly in the teacher's angle of view.
The families were phoned weekly to check for any potential issues with the FM system and CI. Students who experienced technical problems were invited to the clinic for control procedures. Parents and teachers were also asked to check the FM systems regularly every day.
Achievement tests
The achievement tests for life sciences, mathematics, and Turkish for first grade primary school students were specifically developed for this study through a comprehensive evaluation process including the preparation stage and the stages of the validity and reliability.
In the first stage, we aimed to identify academic difficulties experienced by first grade primary school students with CI. For this purpose, primarily, the classroom and special education teachers teaching children with CI were interviewed. Based on the feedback received during the interviews, issues were listed. These interviews in the first stage revealed that children with CI had difficulties, especially in reading comprehension, expressing the content of the text, listening comprehension, solving math problems, and taking dictation.
In the second stage, we aimed to identify the basic objectives of achievement in the previously listed academic subjects. Basic objectives of achievement were described as "a statement of what the student is expected to know, understand, and/or be able to perform at the end of a period of learning"[29]. We considered that the identified gains by students via the listed courses would form the basis for questions to be developed for the achievement tests. Before developing the achievement tests, the curriculum and guidance booklets developed by the Head Council of Education and Morality of the Turkish Ministry of National Education were reviewed in collaboration with two teachers and a faculty member from the Department of Assessment and Evaluation of the Faculty of Education. The curriculum and guidance booklets covered the targeted gains to be acquired through the Turkish, mathematics, and life sciences curricula for the first grade of the primary school. After reviewing the respective guidelines and booklets, the expected gains were identified. The following points were taken into consideration while selecting the gains to be assessed: 1. Out of the gains serving the same purpose or similar purposes, the optimal one was chosen. 2. Gains that could not be assessed were not included in the achievement tests. 3. Gains that would not directly serve the assessment of the FM system"s contribution on school performance were excluded.
In the third stage, which was the stage of the preparation and selection of questions corresponding to the selected gain items, we utilized a diverse selection of textbooks recommended by the Ministry of Education for the first grade of primary school. The order of the questions in the achievement tests was arranged to rank from the easiest to the most difficult one. The same teachers and the same academician, who took part in the previously mentioned tasks, selected the achievement test questions. The following points were taken into consideration while preparing the questions in cooperation with the teachers and the academician, who was an expert in assessment and evaluation: a. The questions were formulated using clear and understandable language. b. the questions were capable of measuring the expected gains.
At the stage of measuring the validity and reliability of the questions prepared (fourth stage), an elementary school was chosen, where normal-hearing students attended. The developed questions were preliminarily administered to a total of 34 second-grade primary school students from two different classes in the first week of school. As per the problems detected during and after the preliminary administration of the questions, respective questions were revised to eliminate potential misunderstandings of students. The reliability of the developed test was assessed by calculating the KR-20 reliability coefficient. Item discriminations were assessed by calculating the item-test correlations using the point biserial correlation coefficient. Items that did not have sufficient discrimination value (<0.20) were excluded from the test based on the results of the analyses[30-33]. The tests were finalized after consulting with the same teachers and the same academician, who took part in the previous procedures. The reliability coefficients calculated for the tests ranged from 0.74 to 0.86. This value was observed to be higher than 0.70, which was accepted as the lower limit of reliability for achievement tests[33,34]. After the revisions, it was concluded that the questions in the achievement tests were suitable for measuring the students' success level.
In the fifth stage, the achievement test questions on life sciences, mathematics, and Turkish were collected in a single booklet. We prepared these questions to appropriately reflect the gains and ranked them in increasing order of difficulty. Participating children in both groups underwent assessments in a silent room equipped with tools (a video camera, a stopwatch, and data recording forms) to collect data. The Turkish, mathematics, and life sciences achievement tests were administered approximately in 35, 15, and 10 min, respectively. Assessments of the participants' school performance level covered one academic year. The tests were administered to participants at the beginning of the year and in 3-month intervals (+1/-1 weeks) during the academic year. A total of four assessments were performed. During the administration of the achievement tests, the FM systems of the CI + FM group participants were switched off.
The correct answer of each question in the achievement test on each of the academic courses was scored by the degree of difficulty. The scoring was conducted in collaboration with experts and the assessment specialist according to the level of representing scope of the questions.
Determination of the teacher factor and school readiness levels of normal-hearing children in both groups
A total of 67 normal-hearing children attending the same class with the participants of both groups were selected randomly at the study baseline to exclude a potential teacher factor and determine the differences between the school readiness levels of the normal-hearing children. The normal-hearing children were assessed through the same achievement tests but only twice; one at baseline and the other at the end of the study period. There were no significant differences between normal-hearing peers in both groups regarding the achievement test score averages in the first and fourth assessments based on the independent samples t-test results (p> 0.05).
Statistical Analysis
The differences in demographical characteristics between the two groups were analyzed using the Mann-Whitney U test. The effect of using the FM system on the school performance level of first grade primary school students with CI was determined using the variance in repeated measures. The pre-test and post-test mean changes by the groups were analyzed with the unrelated samples t-test. Considering the reference studies, the p value was determined as 0.05 in the study[35]. Statistical analyses were performed using SPSS version 15.0.
Results
The assessments were performed for the two groups at the beginning of the study, in the third month, in the sixth month, and in the ninth month. The first, second, third, and fourth assessments were named as the "1st assessment", "2nd assessment" "3rd assessment", and the "4th assessment", respectively.The means of four scores obtained from all achievement tests (life sciences, mathematics, and Turkish) are presented by the groups in Table 2. According to Table 2, the CI + FM group's mean scores obtained from all achievement tests were significantly higher than those of the CI group as of the second assessment.
){kind=link}
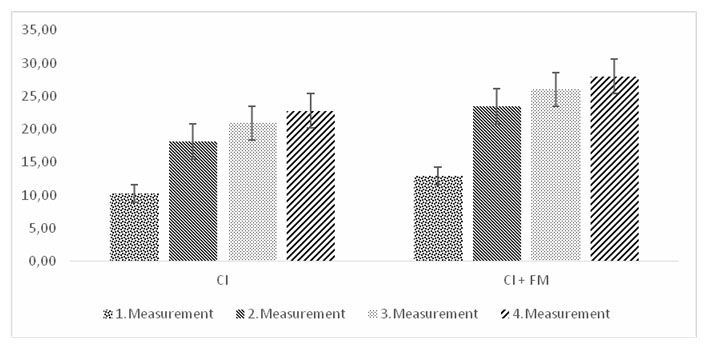
A two-factor ANOVA test was performed to determine both intragroup and intergroup changes in the mean scores of the achievement tests in the CI and CI + FM groups over time (from the 1st to the 4th assessment). A statistically significant increase was observed in the mean scores (test performance) of both groups in the life sciences achievement test over time [F(3.45) = 164.207, p<0.05]. The mean scores of the CI + FM group were higher than those of the CI group (Figure 1) from baseline to the last assessment (group-measurement effect) but no statistically significant differences were observed between the mean scores of the two groups (intergroup difference) [F(3.45) = 1.845, p = 0.153 (p>0.05)].
 Büyütmek İçin Tıklayın |
Figure 1: Life science lesson achievement test- repeated measurement scores for CI and CI+FM groups |
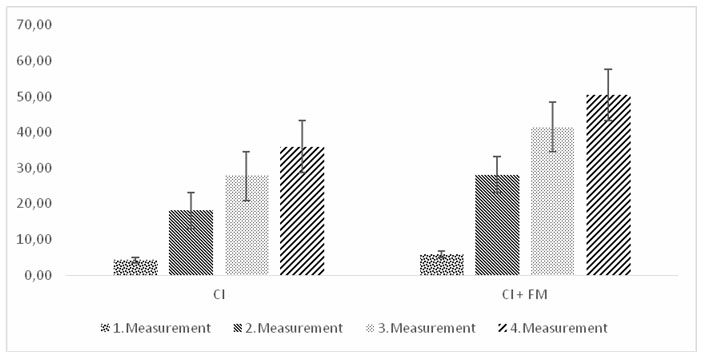
A statistically significant increase was found in the mean scores of the mathematics achievement test in both groups over time [F(3.45) = 88.743, p<0.05]. A statistically significant difference was found in the mean scores of the two groups from baseline to the last assessment (group-measurement effect) [F(3.45) = 2.813, p <0.05)] (Figure 2), meaning that the performance of the CI + FM group in the mathematics achievement test significantly increased over time compared to the CI group.
 Büyütmek İçin Tıklayın |
Figure 2: Mathematics lesson achievement test- repeated measurement scores for CI and CI+FM groups |
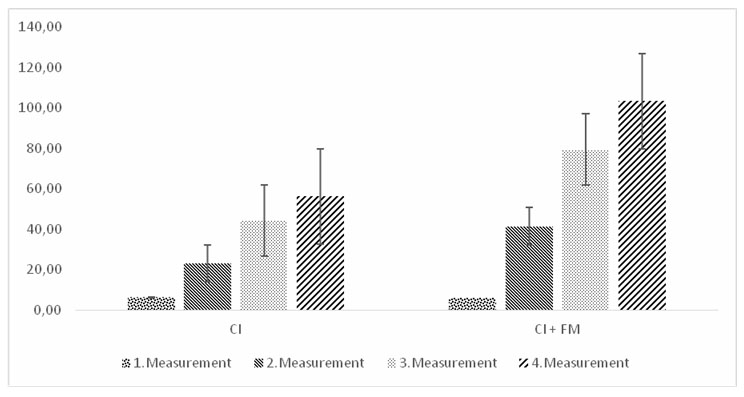
The mean scores of both groups increased statistically significantly from the 1st assessment to the 4th assessment in the Turkish achievement test [F(3.45) = 48.144, p<0.05)]. The comparison between the CI + FM and CI groups revealed a significant difference in the increase of the test scores of the two groups (intergroup difference) from baseline to the last assessment [F(3.45) = 4.862, p<0.05) (Figure 3)], demonstrating that the increase in the CI+FM group's test performance in Turkish was significantly higher over time compared to the CI group.
 Büyütmek İçin Tıklayın |
Figure 3: Turkish Lesson Achievement Test-Repeated Measurement Scores for CI and CI+FM Groups |
Discussion
Studies have shown that cochlear implantation provides speech perception, production, and speech-language[36-38]. However, CI is not sufficient to develop academic skills such as reading and writing. Listening assistive devices such as FM systems may be needed[24]. We aimed to analyze the effect of personal FM system use on the school performance of children with CI in primary school first grade, where mainly verbal communication takes place.In our study, a statistically significant increase was observed over time in the mean scores of all achievement tests in both groups (Table 2). The difference between the first and the last assessments was significant. The mean age of undergoing cochlear implantation surgery was younger than 31 months in the overall group of the study participants. Besides, participants started receiving audio-verbal training early in special education centers. These factors were thought to contribute to the statistically significant improvements in the scores of all achievement tests obtained over time in both groups. Marschark et al. critically analyzed experimental studies investigating literacy and other areas of academic achievements in children with CI[39]. In such experimental studies, because of the improvements in speech production, speech perception, language, literacy, and social development in children undergoing early cochlear implantation surgery, similar improvements have been observed in academic achievements, too.
In a study investigating diverse aspects of mathematical skills including arithmetic, counting, and geometrical reasoning in children with CI, the performance of children with CI was found significantly lower compared to the control group[40]. This finding was explained by insufficient language development rather than an insufficiency in mathematical skills, considering that teaching mathematics requires narratives via complex verbal explanations. Similarly, other studies which reported poor mathematical performance in children with hearing loss have also associated the results with poor language skills[41-43]. Davis reported that children with hearing disability might have disadvantages in interpreting mathematical information successfully and using symbols in a mathematical context because of the level of development in communication skills[44]. Therefore, ensuring the ease of communication in the learning environment is of marked importance for children with hearing loss. Poor access to sound can cause academic delays in children with hearing loss. In particular, noise is considered to have a detrimental effect on learning and achievement in primary school children. Shield and Dockrell found a significant and negative correlation between noise levels and math skills in primary school children[6]. In our study, the increase in the mean scores of the mathematics achievement test over time was statistically significantly higher in the CI + FM group compared to the CI group. This finding demonstrates that long-term use of FM systems in combination with CI reduces the effect of noise and enables students to understand the teacher's verbal instructions and mathematical topics clearly in the classroom environment.
The Turkish language achievement test in our study comprised questions related to verbal reading, dictation skills, reading comprehension, and listening abilities. In the CI + FM group, the average scores obtained from the Turkish language achievement test significantly increased more from the first to the last assessment compared to the CI group. Shield and Dockrell found that the performance of primary school children in reading and mathematics was unfavorably affected by the classroom speech noise compared to quiet situations[6]. In a review study by Klatte et al., it was reported that children exposed to classroom noise and reverberation performed poorly in verbal tasks and had poor reading performance[45]. It was observed that noise was much more likely to impair tasks associated with speech perception and listening comprehension in children than adults. Non-auditory tasks such as short-term memory, reading, and writing were affected by noise, too. Furthermore, classroom learning activities are expected to improve the development of the spoken language and to enable the child to understand more complex sentences compared to the sentences used in daily life. Reading skills and literacy have been found to be related to spoken language. Therefore, children with poor spoken language skills can be predicted to be at risk of reading difficulties. It was reported that, although CI enhanced the auditory capacity, inadequacies in language and literacy might persist. Therefore, the importance of early cochlear implantation has been stressed[46]. In our study, we thought that the increase in the average scores obtained from the Turkish language achievement test in both the CI and the CI+FM groups as of the second assessment paralleled the improved language skills of the students because of early cochlear implantation surgery and special education support services. In the study, teachers taught using the auditory-verbal method in a typical ordinary classroom environment where the S/N ratio was insufficient. Therefore, it was thought that the CI+FM group achieved higher performance in the Turkish language test compared to the CI group because of the FM system's contribution.
Most topics in life sciences in the primary school curriculum are based on daily life and past experiences. The students participating in the study started receiving literacy skill training in special education centers before starting primary school. This early training might be the reason for the occurrence of the insignificant difference between the CI + FM group and the CI group. Therefore, it can be assumed that these factors could be more effective in the classroom compared to listening skill levels.
Only first-grade primary school students took part in our study. One reason is that the achievement tests developed in our study only aimed at assessing the first-grade level. In addition, a student starting the first grade does not yet have a background in Turkish, Mathematics, and Life Sciences, other than the knowledge learned in kindergarten. Therefore, in this study, it was aimed to exclude the effect of previously acquired academic knowledge to show the effect of the FM system on academic achievement and progress more clearly. The assessments during the entire academic year and the inclusion of children, who had just started primary school, provided the opportunity to evaluate better the effects of the FM system on school performance.
Our study investigated the effect of the personal FM system on the school performance of first-grade primary school students assessed via achievement tests in three-month intervals, covering one academic year. In this sense, our study is the first in the literature to evaluate the long-term contributions of the use of personal FM systems to the academic performance of first-grade primary school children with CI via achievement tests, proven to be valid and reliable. There are a limited number of studies in the literature evaluating the short-term benefits of the FM system in the classroom setting in children with hearing loss in different age ranges[18,26,47]. However, these studies have not directly analyzed the relationship between the FM system and school performance. They mostly focused on the FM system's positive contributions to the amelioration of the difficulties in speech recognition and speech perception experienced by students in the presence of background noise in the classroom environment.
Study Limitations
The findings in our study are of importance for educational settings and school performance of children with CI. However, our study has a few limitations. The results of our study should be considered preliminary because a larger study sample and a longer period of assessments are needed to better evaluate the effects of the FM system in educational settings and daily life including the home environment. On the other hand, subjective evaluations of teachers and parents regarding the benefits of the FM system should also be evaluated besides the objective achievement tests developed for the study.
In conclusion, this is the first study evaluating the FM system's effectiveness over a year on achievement test scores of first-grade primary school students with CI. It was found that the use of the FM system contributed to the school performance of the first grade primary school students in the classroom. Therefore, this result supports the need for the use of an FM system in the school environment in students with hearing loss. To establish best practice guidelines for the fitting and adjustment of these devices and to support the contribution of ALD in an educational environment, further studies are needed to explore specific barriers and facilitators in the acquisition and use of ALD for hearing-impaired children.
Conflicts of interest/competing interests: All authors declare that they have no conflict of interest.
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Acknowledgments: This paper is adapted from the MSc thesis in audiology.
Reference
1) Francis HW, Koch ME, Wyatt JR, Niparko JK. Trends in educational placement and cost-benefit considerations in children with cochlear implants. Arch Otolaryngol Head Neck Surg. 1999;125(5):499-505. doi:10.1001/archotol.125.5.499 [ Özet ]
2) Sorkin DL, Zwolan TA. Trends in educational services for children with cochlear implants. Elsevier. 2004;127, 417-21. doi.org/10.1016/j.ics.2004.08.066
3) Houston DM, Miyamoto RT. Effects of early auditory experience on word learning and speech perception in deaf children with cochlear implants: implications for sensitive periods of language development. Otol Neurotol. 2010;31(8):1248-1253. doi:10.1097/MAO.0b013e3181f1cc6a [ Özet ]
4) Percy-Smith L, Jensen JH, Josvassen JL, et al. Foraeldrevurdering af talesprog og generel trivsel hos børn med cochleaimplantat [Parents' perceptions of their deaf children's speech, language and social outcome after cochlear implantation]. Ugeskr Laeger. 2006;168(33):2659-2664. [ Özet ]
5) Schafer EC, Thibodeau LM. Speech recognition in noise in children with cochlear implants while listening in bilateral, bimodal, and FM-system arrangements. Am J Audiol. 2006;15: 114-126. doi:10.1044/1059-0889(2006/015) [ Özet ]
6) Shield BM, Dockrell JE. The effects of environmental and classroom noise on the academic attainments of primary school children. J Acoust Soc Am. 2008;123(1):133-144. doi:10.1121/1.2812596 [ Özet ]
7) Nelson PB, Soli S. Acoustical Barriers to Learning: Children at Risk in Every Classroom. Lang Speech Hear Serv Sch. 2000;31(4):356-361. doi:10.1044/0161-1461.3104.356 [ Özet ]
8) Bradlow AR, Kraus N, Hayes E. Speaking clearly for children with learning disabilities: sentence perception in noise. J Speech Lang Hear Res. 2003;46(1):80-97. doi:10.1044/1092-4388(2003/007) [ Özet ]
9) Duchesne L, Sutton A, Bergeron F. Language achievement in children who received cochlear implants between 1 and 2 years of age: group trends and individual patterns. J Deaf Stud Deaf Educ. 2009;14(4):465-485. doi:10.1093/deafed/enp010 [ Özet ]
10) Geers AE, Sedey AL. Language and verbal reasoning skills in adolescents with 10 or more years of cochlear implant experience. Ear Hear. 2011;32(1 Suppl):39S-48S. doi:10.1097/AUD.0b013e3181fa41dc [ Özet ]
11) Spencer LJ, Gantz BJ, Knutson JF. Outcomes and achievement of students who grew up with access to cochlear implants. Laryngoscope. 2004;114(9):1576-1581. doi:10.1097/00005537-200409000-00014 [ Özet ]
12) Wu CM, Liu TC, Liao PJ, Chen CK, Chang BL, Lin BG. Academic achievements and classroom performance in Mandarin-speaking prelingually deafened school children with cochlear implants. Int J Pediatr Otorhinolaryngol. 2013;77(9):1474-1480. doi:10.1016/j.ijporl.2013.06.012 [ Özet ]
13) Venail F, Vieu A, Artieres F, Mondain M, Uziel A. Educational and employment achievements in prelingually deaf children who receive cochlear implants [published correction appears in Arch Otolaryngol Head Neck Surg. 2010;136(6):575]. Arch Otolaryngol Head Neck Surg. 2010;136(4):366-372. doi:10.1001/archoto.2010.31 [ Özet ]
14) Caldwell A, Nittrouer S. Speech perception in noise by children with cochlear implants. J Speech Lang Hear Res. 2013;56(1):13-30. doi:10.1044/1092-4388(2012/11-0338) [ Özet ]
15) Fetterman BL, Domico EH. Speech recognition in background noise of cochlear implant patients. Otolaryngol Head Neck Surg. 2002;126(3):257-263. doi:10.1067/mhn.2002.123044 [ Özet ]
16) Schafer EC, Thibodeau LM. Speech recognition abilities of adults using cochlear implants with FM systems. J Am Acad Audiol. 2004;15(10):678-691. doi:10.3766/jaaa.15.10.3 [ Özet ]
17) Ehrlich G. New classroom acoustics standard- ANSI S12.60-2002. Arlington, VA: Wyle Laboratories, 2003.
18) Flynn T, Flynn M, Gregory M. The FM advantage in the real classroom. J Educ Audiol. 2005: 37-44.
19) Crandell CC, Smaldino JJ. Classroom Acoustics for Children With Normal Hearing and With Hearing Impairment. Lang Speech Hear Serv Sch. 2000;31(4):362-370. doi:10.1044/0161-1461.3104.362 [ Özet ]
20) Anderson KL, Goldstein H. Speech perception benefits of FM and infrared devices to children with hearing aids in a typical classroom. Lang Speech Hear Serv Sch. 2004;35: 169-184. doi:10.1044/0161-1461(2004/017) [ Özet ]
21) Wolfe J, Schafer EC. Optimizing the benefit of sound processors coupled to personal FM systems. J Am Acad Audiol. 2008;19:585-594. doi:10.3766/jaaa.19.8.2 [ Özet ]
22) Choi JE, Hong SH, Moon IJ. Academic Performance, Communication, and Psychosocial Development of Prelingual Deaf Children with Cochlear Implants in Mainstream Schools. J Audiol Otol. 2020;24(2):61-70. doi:10.7874/jao.2019.00346 [ Özet ]
23) Hawkins DB. Comparisons of speech recognition in noise by mildly-to-moderately hearing-impaired children using hearing aids and FM systems. J Speech Hear Disord. 1984;49(4):409-418. doi:10.1044/jshd.4904.409 [ Özet ]
24) Anderson K, Goldstein H, Colodzin L, Iglehart F. Benefit of S/N enhancing devices to speech perception of children listening in a typical classroom with hearing aids or a cochlear implant. J Educ Audiol. 2005;12: 14-28.
25) Schafer E, Kleineck M. Improvements in speech recognition using cochlear implants and three types of fm systems: a meta-analytic approach. J Educ Audiol. 2009;15:4-14
26) Zanin, J., & Rance, G. (2016). Functional hearing in the classroom: assistive listening devices for students with hearing impairment in a mainstream school setting. Int J Audiol, 55(12), 723-729. https://doi.org/10.1080/14992027.2016.1225991 [ Özet ]
27) Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175-191. doi:10.3758/bf03193146 [ Özet ]
28) Johnston KN, John AB, Kreisman NV, Hall JW 3rd, Crandell CC. Multiple benefits of personal FM system use by children with auditory processing disorder (APD). Int J Audiol. 2009;48(6):371-383. doi:10.1080/14992020802687516 [ Özet ]
29) Donnelly R, Fitzmaurice M. Designing Modules for Learning. In: O"Neill, G., Moore, S. and McMullin, B., ed. Emerging Issues in the Practice of University Learning and Teaching, All Ireland Society for Higher Education, Dublin, 2005.
30) Gronlund N. Measurement and Evaluation in Teaching. New York: MacMillan, 1971.
31) Haladyna T, Downing S. Handbook of Test Development. In: Haladyna T, Downing S, editors. Educational Psychology Handbook. Mahwah, New Jersey: Taylor & Francis, 2011.
32) Osterlind S. Constructing Test Items: Multiple-Choice, Constructed-Response, Performance and Other Formats. Netherlands: Springer, 1998.
33) Turgut M, Baykul Y. Eğitimde ölçme ve değerlendirme. Ankara: Pegem Akademi, 2011.
34) Haladyna T. Developing and validating multiple-choice test items: Lawrence Erlbaum Associates, 2004.
35) Abbott EF, Serrano VP, Rethlefsen ML, et al. Trends in P Value, Confidence Interval, and Power Analysis Reporting in Health Professions Education Research Reports: A Systematic Appraisal. Acad Med. 2018;93(2):314-323. doi:10.1097/ACM.0000000000001773 [ Özet ]
36) Archbold SM, Nikolopoulos TP, Tait M, O'Donoghue GM, Lutman ME, Gregory S. Approach to communication, speech perception and intelligibility and pediatric cochlear implantation. Br J Audiol. 2000; 3: 257-64.
37) Thoutenhoofd ED, Archbold SM, Gregory S, Lutman M, Nikolopoulos T, Sach T. Paediatric cochlear implantation: evaluating outcomes. Whurr, 2005.
38) Choi JE, Hong SH, Moon IJ. Academic Performance, Communication, and Psychosocial Development of Prelingual Deaf Children with Cochlear Implants in Mainstream Schools. J Audiol Otol. 2020;24(2):61-70. doi:10.7874/jao.2019.00346 [ Özet ]
39) Marschark M, Rhoten C, Fabich M. Effects of cochlear implants on children's reading and academic achievement. J Deaf Stud Deaf Educ. 2007;12: 269-282. doi:10.1093/deafed/enm013 [ Özet ]
40) Edwards A, Edwards L, Langdon D. The mathematical abilities of children with cochlear implants. Child Neuropsychol. 2013;19: 127-142. doi:10.1080/09297049.2011.639958 [ Özet ]
41) Kelly RR, Lang HG, Pagliaro CM. Mathematics word problem solving for deaf students: a survey of practices in grades 6-12. J Deaf Stud Deaf Educ. 2003;8: 104-119. doi:10.1093/deafed/eng007 [ Özet ]
42) Davis SM, Kelly RR. Comparing deaf and hearing college students' mental arithmetic calculations under two interference conditions. Am Ann Deaf. 2003;148: 213-221. doi:10.1353/aad.2003.0018 [ Özet ]
43) Piştav Akmeşe P, Kol G, Kirazlı G, Suner A, Öğüt F. İşitme kayıplıve normal işiten okul öncesi dönem çocukların erken matematiksel akıl yürütme becerilerinin karşılaştırılması. Erken Çocukluk Çalışmaları Dergisi. 2020; 4:197-221.
44) Davis B. Teaching mathematics: Toward a sound alternative. New York: Garland Publishing; 1996.
45) Klatte M, Bergström K, Lachmann T. Does noise affect learning? A short review on noise effects on cognitive performance in children. Front Psychol. 2013;4: 578. doi:10.3389/fpsyg.2013.00578 [ Özet ]
46) Boothroyd A, Boothroyd-Turner D. Postimplantation audition and educational attainment in children with prelingually acquired profound deafness. Ann Otol Rhinol Laryngol Suppl. 2002;189: 79-84. doi:10.1177/00034894021110s517 [ Özet ]
47) Silva JM, Pizarro LM, Tanamati LF. Use of FM System in cochlear implant. Uso do Sistema FM em implante coclear. Codas. 2017;29: e20160053. doi:10.1590/2317-1782/20172016053 [ Özet ]