


TYMPANIC MEMBRANE TEMPERATURES OF VERTIGINOUS PATIENTS
2Demiroğlu Bilim Üniversitesi, Tıp Fakültesi, İstanbul, Turkey
3İstanbul Florence Nightingale Hastanesi, Kulak Burun Boğaz, İstanbul, Turkey
Summary
Objective: This study aimed to determine the differences between the right and left ear temperatures of patients with vertigo. It also aimed to correlate the results in order to develop definitions for the pathophysiology of the diseases based on the data. Thus, we designed a study to record bilateral tympanic membrane temperatures on 137 vertiginous patients who were seen at our vertigo clinic.Materials and Methods: The study was carried out in patients who applied to Istanbul Florence Nightingale Hospital Ear, Nose and Throat Diseases Clinic with the complaint of dizziness. After confirming that there was no abnormality in the otoscopic examination, the temperature of both ears were measured with a thermometer, prior to the vestibular examination being carried out in the vestibular laboratory with the presumptive diagnosis of true vertigo. The data recorded include the patient's demographic information, examination findings, and the results obtained from the vestibular laboratory. Mean, standard deviation, median, minimum, maximum value frequency, and percentage were used for descriptive statistics.
Results: A total of 137 patients were included in the study. No significant (p > 0.05) difference was observed between pathologic Side and other Side measurements in the benign paroxysmal positional vertigo (BPPV) group, Ménière's disease group, or vestibulopathy group. Nystagmus at presentation in the group without otologic pathology, i.e. those patients without overt vestibular pathology, was significantly (p < 0.05) higher than in the BPPV, Meniere's, or vestibulopathy groups.
Conclusion: Our study failed to disclose any significant difference of tympanic membrane temperatures in patients with vertiginous complaints.
Introduction
Vertigo presents as a sensation of movement of the environment around the patient, affecting their quality of life. Vertigo is a commonly encountered symptom in clinical practice and emergency rooms, and has an estimated lifetime prevalence of up to 10%. [1] Vertigo is caused by a lesion affecting the vestibular pathways at any point from the labyrinth to the vestibular nuclei or its central connections. [2]The etiology of vertigo generally consists of either central or peripheral causes. The common causes of vertigo seen in primary care are benign paroxysmal positional vertigo (BPPV), vestibular neuronitis, vestibular migraine (VM), and Ménière's disease. [3-5] It is possible that the key mechanism of vertigo in migraine is related to the sterile inflammation of intracranial vessels, vasodilatation, and plasma extravasation in and around the inner ear. [6] It is also known that vestibular receptors are pressure-sensitive. [7]
One of the diagnostic tests utilized for the differential diagnosis of vertigo, the caloric stimulation test, first described by Robert Barany in 1906, uses changes in ear temperature by applying water or air. [8,9] This diagnostic tool is used to understand the origin of vertigo by causing vertigo in patients in a clinical setting and measuring the response rate of each ear while comparing them to each other.
Caloric testing is the only procedure that assesses each labyrinth separately. It helps find the affected side and provides information about the extent of the vestibular lesion. Caloric stimulation of the labyrinth causes a flow of endolymph within the semicircular canals, which causes polarization or depolarization of the hair cells of the ampulla, which becomes visible through the vestibular-ocular reflex. [10] Caloric testing is most useful for diagnosing certain diseases, including Meniere's disease and VM. [11] The most consistent laboratory finding in VM is a unilaterally reduced caloric response. [6]
Measurement of tympanic membrane temperatures (TMTs) using infrared thermometry has become an invaluable tool for measuring the core body temperature. It has been shown that TMTs demonstrate strong correlations with concurrent temperature measures in the pulmonary artery, rectum, and mouth. [12]
TMT is also accepted as a good index of brain temperature, as its variations reflect changes in brain core temperature. As Propper et al. stated in their study, hemispheric activity affects ear temperature, although the mechanisms by which TMT may be related to hemispheric activity are not completely known. [13,14] TMT is greatly influenced by the internal carotid artery and the jugular vein, and it shows considerable circadian changes parallel to the core body temperature. [15,16] In one study in Japan, the effects of Meniere's disease on ear temperature were shown on one patient whose TMT varied widely after the attack of vertigo. [15]
In this current study, based on the research, we expected to determine the differences between the right and left ear temperatures of vertigo patients, and while correlating the results, to develop definitions for the pathophysiology of the diseases based on this information. Thus, we designed a study to record TMTs on a series of vertiginous patients who were seen at our vertigo clinic.
Methods
This study adheres to the principles of the Declaration of Helsinki. It was carried out in accordance with the Ethics Committee of Demiroğlu Bilim University (Protocol no: 44140529/ 8748, approved on 02.11.2021). Written informed consent was obtained from all patients.
Study design
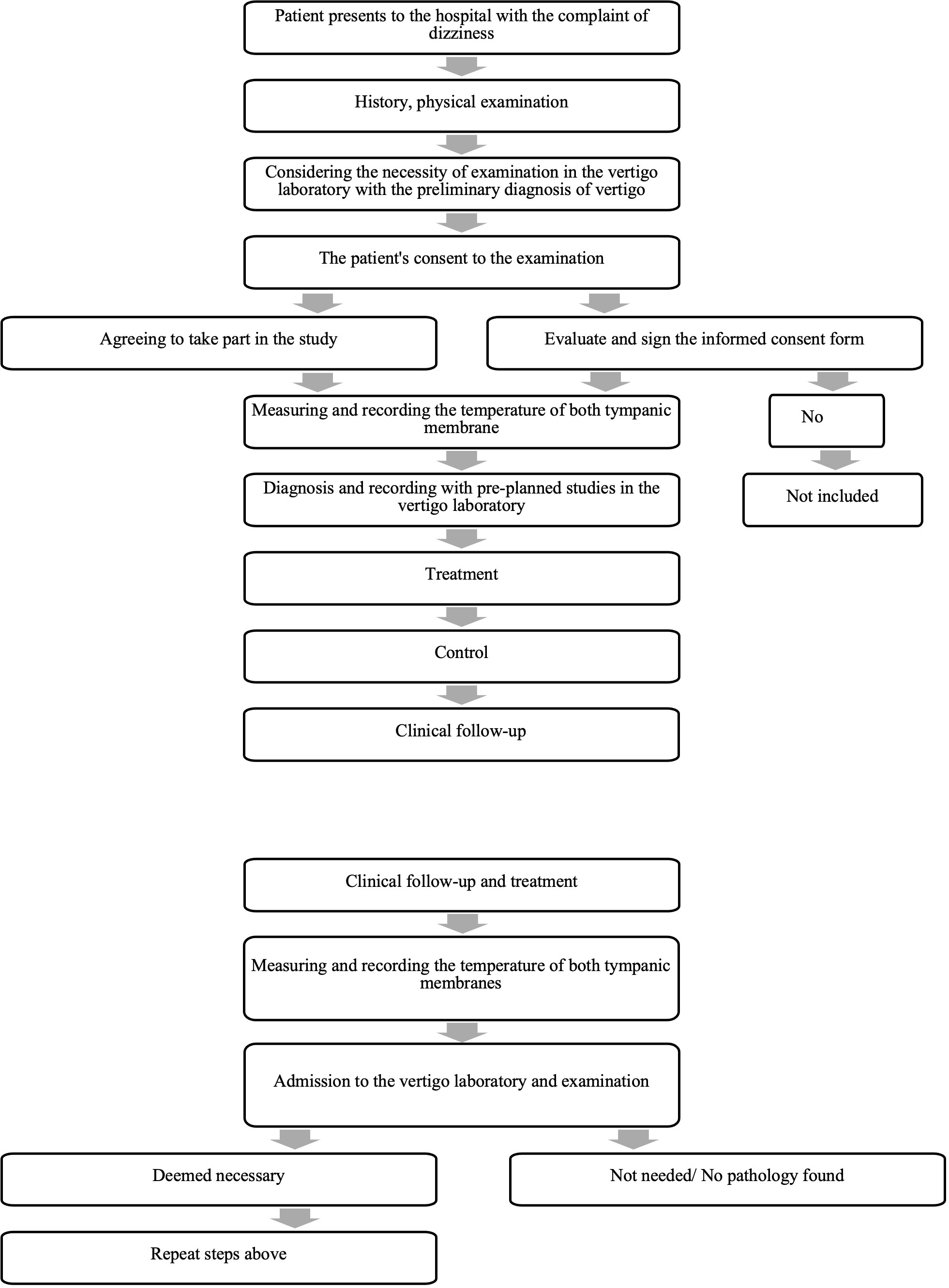
The study was carried out in patients who applied to Istanbul Florence Nightingale Hospital Ear, Nose and Throat Diseases Clinic with the complaint of dizziness. Standard outpatient procedures of the patients were performed, and vertigo-specific inquiries were made in addition to the otoscopic examination. After confirming that there was no abnormality in the otoscopic examination, the temperature of both ears was measured with a thermometer, prior to the vestibular examination being carried out in the vestibular laboratory with the presumptive diagnosis of true vertigo. During the follow-up of these patients, TMTs were measured again. The steps involved in this study are given in a flow chart at Figure 1. The data sought included patient's demographic information, examination findings, and the results obtained from the vestibular laboratory (Table 1). The vestibular laboratory uses Micromedical by Interacoustics Aqua Stim (Interacoustics A/S, Denmark) to examine the following parameters: spontaneous nystagmus, Dix-Hallpike maneuver, supine roll, gaze horizontal, gaze vertical, saccade random, pursuit, and optokinetic fixed. A Genius 2 (Covidien, Ireland) tympanic temperature measuring device was used to measure TMTs. The measurements were taken with the patient seated in a chair and prior to any caloric testing. The same thermometer was used for each patient to ensure consistency in ear temperature measurement, and the calibration of the measuring instrument was checked regularly by the department of Biomedical Engineering of the hospital.
){kind=link}
 Büyütmek İçin Tıklayın |
Figure 1: The Flow Chart of The Study |
Study group
The study group involved adult patients who applied to the Istanbul Florence Nightingale Hospital Ear Nose and Throat Department with the complaint of dizziness between 15 November 2021 and 30 April 2022. A patient was excluded from the study if there were no findings compatible with true vertigo that required examination in the vestibular laboratory, or if the patient did not want to volunteer, had a febrile or infectious disease, or the tympanic membrane and otoscopic findings were not within the normal limits.
Statistical analysis
Mean, standard deviation, median, minimum, maximum value frequency, and percentage were used for descriptive statistics. The distribution of variables was checked with a Kolmogorov-Smirnov test. ANOVA, Kruskal-Wallis and Mann-Whitney U tests were used to compare quantitative data. A Wilcoxon test was used for the repeated measurement analysis and a Chi-Square test was used for the comparison of qualitative data. SPSS 28.0 was used for statistical analyses.
Results
A total of 137 patients were included in the study. Patients' distribution according to age, gender, and pathology are given in Table 2. The presence vs. absence of significant medical issues and/or physical findings were noted as well and are given in Table 3.){kind=link}
){kind=link}
Table 2: Patients' distribution according to age, gender, and pathology.
Table 3: The presence vs. absence of significant medical issues and/or physical findings
Patients were grouped according to their clinical diagnosis. The clinical diagnoses were established according to the patient's history, physical findings (presence or absence of nystagmus), and the results obtained from the vestibular laboratory. These diagnoses were then grouped by BPPV, Meniere's disease, vestibulopathy, and no vestibular pathology. The term vestibulopathy was used for cases where it was not possible to make a clear diagnosis, however patients" findings were highly suggestive of a vestibular pathology, with a significant portion of them possibly having either Meniere's disease without cochlear symptomatology or vestibular neuritis.
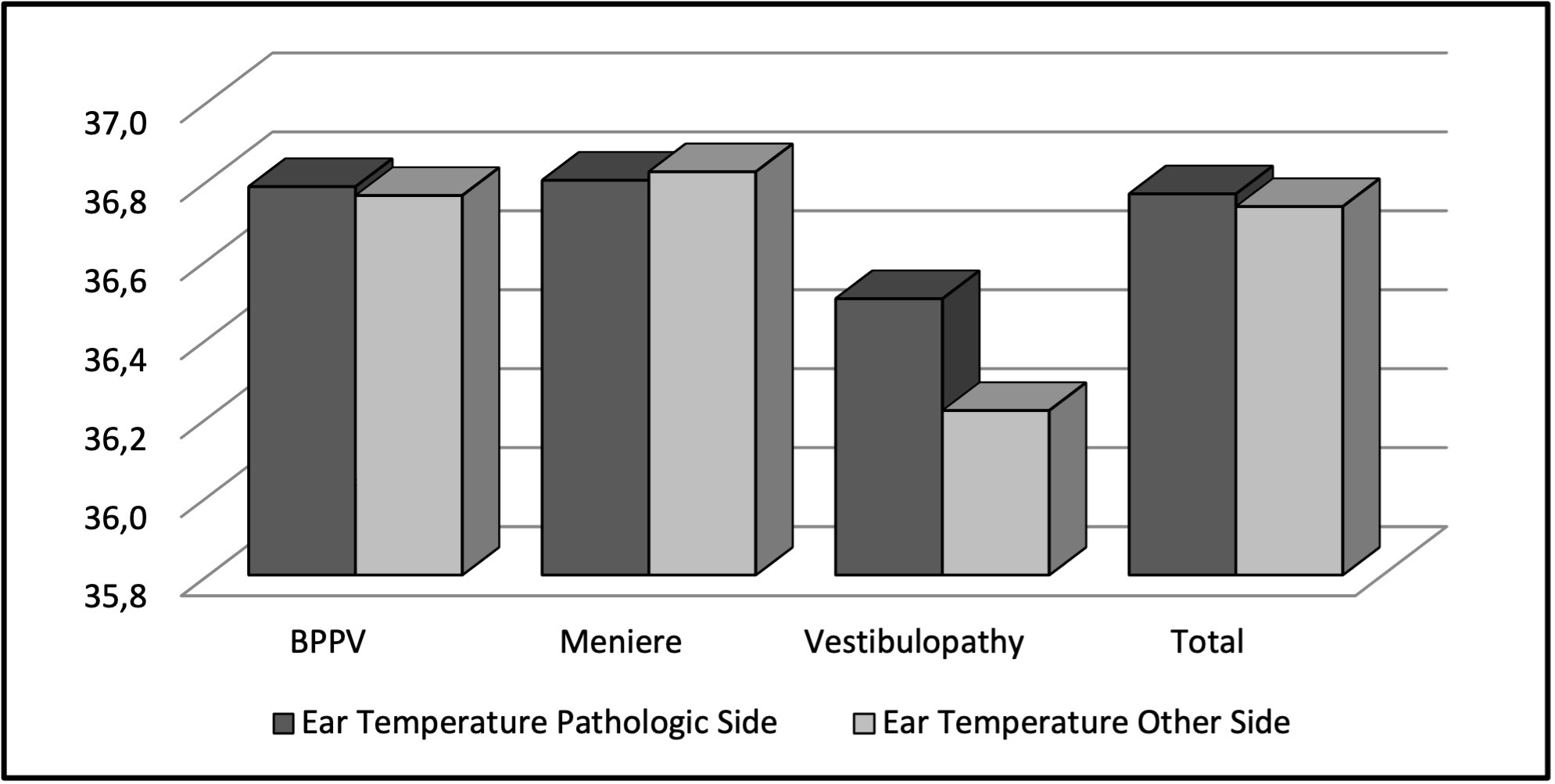
These groups were then compared according the temperature values obtained. No significant (p > 0.05) difference was observed between the Pathologic Side and other Side measurements in the BPPV group, the Meniere's group (p > 0.05), or the vestibulopathy group. No significant (p > 0.05) difference was observed between the Pathologic Side and other Side measurements in all patient groups (Table 4 and Figure 2).
){kind=link}
Table 4: Comparison of ear temperatures according to the pathology side vs. normal ear.
 Büyütmek İçin Tıklayın |
Figure 2: Chart demonstrating ear temperature differences according to the pathology. |
There was no significant difference (p > 0.05) between the non-pathological, BPPV, Meniere's, and vestibulopathy groups in terms of age, gender distribution, general medical history, or history of ear problems (Table 5).
){kind=link}
Table 5: General distribution of patients
Nystagmus at presentation in the group without pathology was significantly (p < 0.05) lower than in the BPPV, Meniere's, and vestibulopathy groups. This group of patients with nystagmus at presentation, though without vestibular pathology, was considered to be consisting of patients with a possible neurologic disorder. These patients were later referred to the neurology department. The nystagmus at presentation rate in the BPPV group was significantly (p < 0.05) lower than in the Meniere's and vestibulopathy groups (
Discussion
True vertigo is most likely caused by a disorder of the vestibular system, which is a sensory system comprised of sensory transducer organs in the inner ear with its three orthogonal semicircular canals and two otolith organs. [17]Research shows that the vestibular system is sensitive to thermal stimuli, which has become one of the commonly used vestibular tests through bithermal caloric testing. [9,18] As such, this test is utilized for diagnostic purposes of peripheral vestibular disorders, such as Meniere's disease, VM, vestibular neuritis, as well as for central vestibular disorders, such as multiple sclerosis, and lacunar infarcts. [19]Researchers who have done postmortem studies have postulated that Meniere's disease is associated with an increase of the endolymph within the inner ear membranous labyrinth, yet not all cases of increased endolymph produce the same clinical picture, leaving part of the pathogenesis yet to be discovered. [3] The cause of another vestibular disorder, VM, also remains unclear. [6]
TMT has been in clinical use for several decades. [20] It has been shown that the major supplier of the ear drum's vascularization is the external carotid artery, however a proportion would be derived from the internal carotid artery. That artery perfuses both the hypothalamus, which is involved in psychobiological stress responses, and the frontal cortex, which is involved in the processing of emotional information. [12,21]
TMT was also found to represent a measure of the temperature of proximal brain tissue and possibly hemispheric activation. [13,22,23] It is accepted that an absolute difference between left and right TMT is indicative of relative hemispheric activation. [13] According to Helton, a consistent elevated temperature in ipsilateral ear drum can reflect cortical temperature, overall resting state, or residual activation in the ipsilateral hemisphere. [24] TMT measures have been associated with lateralized cognitive and emotional/motivational states, including fear and stress. [16,25,26,27]
The absolute mechanisms by which TMT may be related to hemispheric activity are not completely known. [13] In one study, researchers found evidence for a link between increased TMT and increased ipsilateral hemispheric activation after mood-induction. [13] Another explanation is that decreased TMT is thought to be associated with increased hemispheric activation on the ipsilateral side of the brain. As the ipsilateral carotid artery is the main source of ipsilateral hemisphere and tympanic membrane, the same side skull and related structures demonstrate characteristics of heat dissipation. The blood flow around the tympanic membrane is thought to be cooler than blood being actively recruited by the brain during neuronal activity; in other words, increased hemispheric activity is associated with decreased TMT ipsilaterally. [24]
Besides the level of the hemispheric activity, TMT might be reflecting other factors locally or might be affected by external issues such as postural changes of the subject, head tilt, age, tympanic membrane pathology, cerumen and excessive hair, humidity, cooling of the face (especially in hyperthermia), cerebrovascular disease (stroke), and cold ambient temperatures. [21,23,26] One single-patient study showed that Meniere's disease had an effect on the patient's TMT after an attack of vertigo. [15]
Our results failed to disclose any relationship between TMT and common vestibular disorders, namely BPPV, Meniere's disease, or unspecified vestibular pathologies. As shown in Table 4 and Figure 2, TMT tended to be higher in the involved ear in the vestibulopathy group; however this difference did not reach statistical significance; more so, the ear that was not involved seemed to have a comparably lower temperature (median 36.3° C) than the ear with the pathology (median 36.6° C).
However, our study has shown that nystagmus at presentation was significantly less common among patients without vestibular pathologies, yet among the vestibular pathologies group, patients with BPPV seemed to have more accounts of nystagmus at presentation compared to the Meniere's disease and vestibulopathy groups. As those patients with a final diagnosis of BPPV originating from lateral semicircular canal were found to have pseudo-spontaneous nystagmus, it is possible to say that nystagmus at presentation was significantly more common among patients with Meniere's disease and vestibulopathy. This is in correlation with the literature. [28] An exception to this theory is that healthy normal controls without vestibular or autonomic symptoms may exhibit low velocity nystagmus. [29]
Our study had some limitations. One limitation could be the reading quality of the device used for measuring TMT. While TMT is accepted as a reliable and accurate method for measuring core temperature, [30] the measurement accuracy is dependent on the correct positioning of the probe. [31] Different ear anatomy and probe designs that are not compliant with the external ear shape might cause some inaccurate readings. [20]
In our study we used a tympanic thermometer which is reportedly highly accurate and which had been regularly checked for functionality and calibrated by our biomedical department. All of the patients had a prior ear examination and cerumen removal if needed, after which the study had started. The patients had all their tests done in a well air conditioned space and the tests were done between 9:00 a.m. and 5.00 p.m. Yet, there might still be factors that affect TMTs that have been missed throughout the study. Another limitation could be the relative absence of further diagnostic tools to help confirm the diagnosis and the relative activity levels of the cerebral hemispheres.
Conclusion
This study failed to find any difference between TMTs of patients with vestibular disorders. Thus, it can be concluded that with the present devices no temperature differences were detected in patients with vertiginous complaints.
Acknowledgments
The authors would like to express their gratitude to Drs. Kristin Joanna Hannavi and Rana Gür for their support throughout data acquisition and literature search of the study.
Reference
1) van de Berg R, Murdin L, Whitney SL, Holmberg J, Bisdorff A. Curriculum for Vestibular Medicine (VestMed) proposed by the Bárány Society: The concept of Vestibular Medicine and the framework defining the knowledge, skills and attitudes needed for proficiency in Vestibular Medicine. VES. 2022 Mar 28;32(2):89-98. [ Özet ]
2) Voetsch B, Sehgal S. Acute Dizziness, Vertigo, and Unsteadiness. Neurologic Clinics. 2021 May;39(2):373-89. [ Özet ]
3) Basura GJ, Adams ME, Monfared A, Schwartz SR, Antonelli PJ, Burkard R, et al. Clinical Practice Guideline: Ménière's Disease Executive Summary. Otolaryngol Head Neck Surg. 2020 Apr;162(4):415-34. [ Özet ]
4) Mallampalli MP, Rizk HG, Kheradmand A, Beh SC, Abouzari M, Bassett AM, et al. Care Gaps and Recommendations in Vestibular Migraine: An Expert Panel Summit. Front Neurol. 2022 Jan 3;12:812678. [ Özet ]
5) Sarna B, Abouzari M, Lin HW, Djalilian HR. A hypothetical proposal for association between migraine and Meniere's disease. Medical Hypotheses. 2020 Jan;134:109430. [ Özet ]
6) Lempert T, von Brevern M. Vestibular Migraine. Neurologic Clinics. 2019 Nov;37(4):695-706. [ Özet ]
7) Gürkov R, Strobl R, Heinlin N, Krause E, Olzowy B, Koppe C, et al. Atmospheric Pressure and Onset of Episodes of Menière's Disease - A Repeated Measures Study. Langguth B, editor. PLoS ONE. 2016 Apr 20;11(4):e0152714. [ Özet ]
8) Choi WY, Gold DR. Vestibular Disorders: Pearls and Pitfalls. Semin Neurol. 2019 Dec;39(06):761-74. [ Özet ]
9) Shaikh AG. A trail of artificial vestibular stimulation: electricity, heat, and magnet. Journal of Neurophysiology. 2012 Jul 1;108(1):1-4. [ Özet ]
10) Barros ACMP de, Caovilla HH. Do nistagmo às provas calóricas com ar e com água. Braz j otorhinolaryngol. 2012 Aug;78(4):120-5. [ Özet ]
11) Yetiser S, Ince D. Caloric Analysis of Patients with Benign Paroxysmal Positional Vertigo. Int Adv Otol. 2017 Dec 21;13(3):390-3. [ Özet ]
12) Boyce WT, Essex MJ, Alkon A, Smider NA, Pickrell T, Kagan J. Temperament, Tympanum, and Temperature: Four Provisional Studies of the Biobehavioral Correlates of Tympanic Membrane Temperature Asymmetries. Child Development. 2002 May;73(3):718-33. [ Özet ]
13) Propper RE, Januszewski A, Brunyé TT, Christman SD. Tympanic Membrane Temperature, Hemispheric Activity, and Affect: Evidence for a Modest Relationship. J Neuropsychiatry Clin Neurosci. 2013; 25:198-204. [ Özet ]
14) Propper RE, Januszewski A, Christman SD, Brunyé TT. Increased Anger is Associated With Increased Hemispheric Asymmetry: Support for Anger-Tympanic Membrane Relationships. Journal of Nervous & Mental Disease. 2011 Sep;199(9):716-20. [ Özet ]
15) Moriya K, Sekitani T, Yamashita H, Mizokami H. Tympanic Membrane Temperature in a Patient With Vertigo. Acta Oto-Laryngologica. 1993 Jan;113(sup506):24-5. [ Özet ]
16) Propper RE, Barr TD, Brunyé TT. Lateralized differences in tympanic membrane temperature, but not induced mood, are related to episodic memory. Brain and Cognition. 2015 Mar;94:52-9. [ Özet ]
17) Ferrè ER, Haggard P. Vestibular cognition: State-of-the-art and future directions. Cognitive Neuropsychology. 2020 Nov 16;37(7-8):413-20. [ Özet ]
18) Ziarati MA, Taziki MH, Hosseini SM. Autonomic laterality in caloric vestibular stimulation. WJC. 2020 Apr 26;12(4):144-54. [ Özet ]
19) Szirmai A, Keller B. Electronystagmographic analysis of caloric test parameters in vestibular disorders. Eur Arch Otorhinolaryngol. 2013 Jan;270(1):87-91. [ Özet ]
20) Yeoh WK, Lee JKW, Lim HY, Gan CW, Liang W, Tan KK. Re-visiting the tympanic membrane vicinity as core body temperature measurement site. Romanovsky AA, editor. PLoS ONE. 2017 Apr 17;12(4):e0174120. [ Özet ]
21) McCarthy PW, Heusch AI. The vagaries of ear temperature assessment. Journal of Medical Engineering & Technology. 2006 Jan;30(4):242-51. [ Özet ]
22) Genovese JEC, Sparks KE, Little KD. Tympanic Membrane Temperature and Hemispheric Cognitive Style. The Journal of Genetic Psychology. 2017 Sep 3;178(5):298-302. [ Özet ]
23) Skaiaa SC, Brattebø G, Aßmus J, Thomassen Ø. The impact of environmental factors in pre-hospital thermistor-based tympanic temperature measurement: a pilot field study. Scand J Trauma Resusc Emerg Med. 2015 Dec;23(1):72. [ Özet ]
24) Helton WS. The relationship between lateral differences in tympanic membrane temperature and behavioral impulsivity. Brain and Cognition. 2010;74:75-78. [ Özet ]
25) Mazzotti GA, Boere V. The right ear but not the left ear temperature is related to stress-induced cortisolaemia in the domestic cat ( Felis catus ). Laterality: Asymmetries of Body, Brain and Cognition. 2009 Mar;14(2):196-204. [ Özet ]
26) Ogawa T, Sugenoya J, Ohnishi N, Natsume K, Imai K, Kandori Y, et al. Effects of body and head positions on bilateral difference in tympanic temperatures. Eur J Appl Physiol. 1993 Oct;67(4):354-9. [ Özet ]
27) Yang WC, Kuo HT, Lin CH, Wu KH, Chang YJ, Chen CY, et al. Tympanic temperature versus temporal temperature in patients with pyrexia and chills. Medicine. 2016 Nov;95(44):e5267. [ Özet ]
28) Baloh RW. Differentiating between peripheral and central causes of vertigo. Journal of the Neurological Sciences. 2004 Jun;221(1-2):3. [ Özet ]
29) Young AS, Rosengren SM, D'Souza M, Bradshaw AP, Welgampola MS. Nystagmus characteristics of healthy controls. VES. 2020 Dec 16;30(6):345-52. 30) Gasim GI, Musa IR, Abdien MT, Adam I. Accuracy of tympanic temperature measurement using an infrared tympanic membrane thermometer. BMC Res Notes. 2013 Dec;6(1):194. [ Özet ]
31) Levander MS, Grodzinsky E. Variation in Normal Ear Temperature. The American Journal of the Medical Sciences. 2017 Oct;354(4):370-8. [ Özet ]