


USAGE OF AUTOMATIC EAR RETRACTOR IN PAROTID SURGERY
2Kahramanmaraş Sütçü İmam Üniversitesi Tıp Fakültesi, KBB, Kahramanmaraş, Turkey
3Kahramanmaraş Sütçü İmam Üniversitesi Tıp Fakültesi, KBB, Kahramanmaraş, Turkey
Summary
Parotidectomy is one of the most commonly performed procedures in ENT practice. Various surgical procedures are performed, ranging from extracapsular dissection of the parotid gland to total parotidectomy.The constant surgical stage in all these procedures is the identification and preservation of the facial nerve. In our clinic, we routinely find and follow the facial nerve from its area of origin: the stylomastoid foramen. During this process, our most important landmark is the tragal pointer. Removal of parotid tissue is essential in exposing this area.The automatic ear retractor used at this stage provides effective, stable and safe retraction. With the usage of this retractor, we believe that the operation time will be reduced and surgery can be performed by less staff. In the Covid-19 pandemic process, shortening the operation time and being able to carry out cases with fewer assistants may be important for both patient and staff safety.Introduction
Parotidectomy requires removing the parotid gland wholly or partially. Parotid gland tumor and metastases to parotid lymphnodes are common indications for this surgical procedure. [1] The anatomy and localization of the facial nerve is the most critical step in parotid gland surgery. The last segment of the nerve exits the skull through the stylomastoid foramen and provides motor innervations for the muscles of facial expression. [2] Facial nerve alteration represents the most important complication resulting in functional and cosmetic deficits. The risk of transient facial nerve dysfunction is estimated to be about 20-40%, while persistent facial nerve palsy occurs in 0-4% of patients. [3] Parotid surgery presents special challenges to the surgeon, because most of the tumors removed are benign and patients commonly expect complete function of the facial nerve after surgery. [1] Extracapsular dissection (ECD), partial lateral parotidectomy, lateral or superficial parotidectomy (SP) and total parotidectomy with preservation of the facial nerve are the different surgical options for treating a benign parotid tumor. [4] Although there are various surgical options for parotid masses, the function and integrity of facial nerve should always be identified and preserved during surgery. Multiple anatomic landmarks have been described for identifying the location of the facial nerve trunk. These landmarks can be listed as digastric muscle, tragal pointer, tympanomastoid fissura, styloid process. Varius clamps such as Allis, Babcock or Langenbeck and Richardson retractors are used but they require usage by surgical assistant. In addition, Hunsaker's article [5] mentions new retractors used in parotidectomy. We use blunt, 3x3 theeth, Laner-Wulstein automatic ear retractor (KLS Martin, Germany) for this purpose. The automatic ear retractor serves the same function without the need for extra staff. Automatic ear retractor is very useful in the stages of revealing the numbered anatomical landmarks, finding and tracking the facial nerve and needs no surgical assistant.In this article, we present our surgical technique that is performed using anautomatic ear retractor to enable identifying facial nerve easily to reduce operation time and number of surgical asistants needed in parotid gland surgery.
Operative technique:
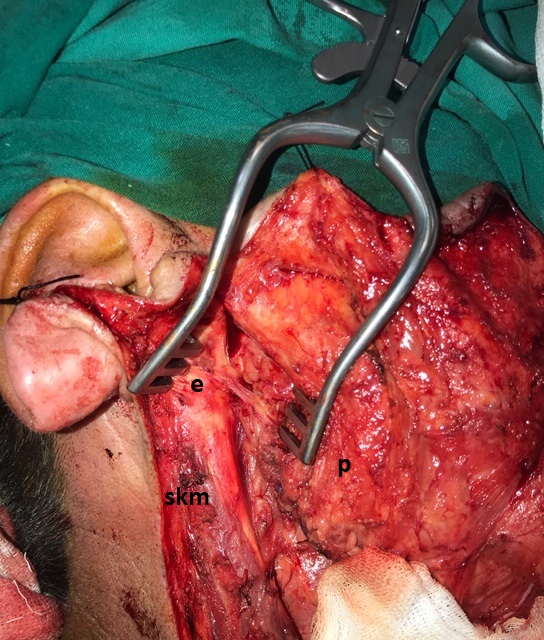
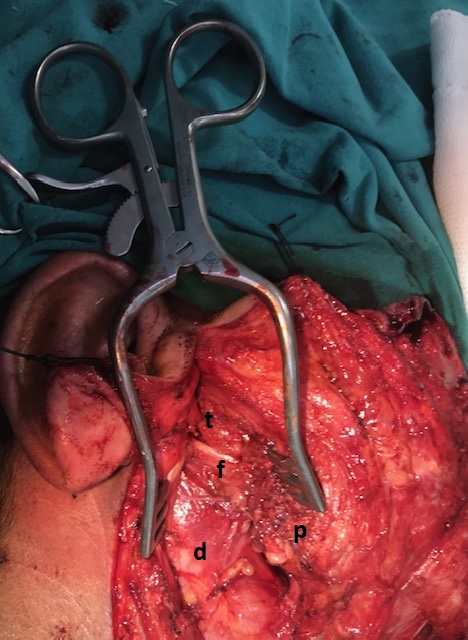
We use modified Blair incision for our routine parotid surgery. The incision should follow the crease just anterior to tragus and curve gently below the earlobe before it becomes almost horizontal in the upper neck about 2 cm below the mandibular angle, preferably along a skin crease. The dissection is carried through the subcutaneous tissues to the just superior to periparotid fascia while avoiding entering the gland or the tumor mass. The flap must raised to the anterior border of the parotid gland. 2-0 silk sutures is place in to earlobe (subcutaneous) for posterior retraction and stay sutures in to the cheek flap for anterior retraction. The anterior border of SCM is skeletonized and separated from the parotid gland. The posterior belly of the digastric muscle is identified by retracting the parotid gland superiorly. Parotid is detached from tragal cartilage with gentle blunt dissection after that we use automatic ear retractor between tragal cartilage and parotid gland. (Figure 1) The tragal pointer is identified by following the cartilaginous external auditory canal medially. After tragal pointer is marked, the retractor is replaced between parotid gland and SCM or tragal cartilage. We are looking for the facial nerve at 1 cm inferomedial of the tragal pointer. In order to confirm the identification of the nerve, we follow it by blunt dissection with a fine haemostat to the point where the nerve splits in two major branches. (Figure 2) We use this retractor for find and track the nerve until we reach the nerve division. This division is termed as pes anserinus and it is a significant surgical landmark. After this stage, facial nerve is dissected meticulously along each nerve branch and mass is excised.
 Büyütmek İçin Tıklayın |
Figure 1: Automatic ear retractor placed between the tragal cartilage and parotid tissue. (p: parotid gland, e: external ear cartilage, scm: sternocleidomastoid muscle) |
 Büyütmek İçin Tıklayın |
Figure 2: Facial nerve can be easily seen by placing the retractor between the SCM and the parotid. (t: tragal pointer, f: facial trunk, p: parotid gland, d: digastric muscle) |
Advantages of this technique:
Automatic ear retractors have been used routinely in parotid surgery in our clinic. This retractor, which we are familiar with as a result of its widespread usage in ear surgeries, is very useful in parotid surgery. The main advantages of this technique are as follows:
1- The automatic ear retractor is an often encountered and easy-to-reach tool for every ENT specialist.
2- A stable and effective retraction is achieved by using this retractor.
3- It is reliable. Blunt-tipped retractors are used and the retractor level lies lateral to the facial nerve.
4- Time taken to find the nerve is reduced due to retactor usage.
5- Surgical procedure can be done with fewer people.
Disadvantages of this technique:
1- Opening the automatic ear retractor excessively may damage the soft tissue and cartilages of the external ear canal.
2- In tumors located close to the tragal cartilage, the retractor may enter the tumor tissue and risks tumour spread.
3- The benefit of this technique is limited in tumors located close to the stylomastoid foramen where the facial nerve trunk is located retrogradely.
In conclusion, automatic ear retractor reduces operation time by facilitating to find the facial nerve. It provides the facility of performing the operation by fewer staff. During the pandemic period, short operation period and the ability to perform the same operation with fewer people are very important for both patient and staff safety. This may also contribute to reduction in operational costs.
Reference
1) Nadershah M, Salama A: Removal of parotid, submandibular, and sublingual glands.Oral and Maxillofacial Surgery Clinics 2012, 24:295-305. [ Özet ]
2) Greywoode JD, Ho HH, Artz GJ, Heffelfinger RN: Management of traumatic facial nerve injuries.Facial Plastic Surgery 2010, 26:511-518. [ Özet ]
3) Mantsopoulos K, Koch M, Klintworth N, Zenk J, Iro H: Evolution and changing trends in surgery for benign parotid tumors.The laryngoscope 2015, 125:122-127. [ Özet ]
4) Quer M, Vander Poorten V, Takes RP, Silver CE, Boedeker CC, de Bree R, Rinaldo A, Sanabria A, Shaha AR, Pujol A: Surgical options in benign parotid tumors: a proposal for classification.European Archives of Oto-Rhino-Laryngology 2017, 274:3825-3836. [ Özet ]
5) Hunsaker DH: A New Set of Parotidectomy Retractors.Otolaryngology-Head and Neck Surgery 1990, 103:497-499. [ Özet ]