


SECOND BRANCHIAL CLEFT ANOMALIES: ANALYSIS OF OUR CLINICAL EXPERIENCE IN 10 YEARS
Summary
Purpose: To review clinical features, the tools used in the diagnosis and the results of surgical treatment of second branchial arch anomalies.Material and Methods: The patients diagnosed with branchial cyst or fistula and managed surgically between January 2008 and December 2018 in the otolaryngology department of a tertiary academic center were reviewed retrospectively.
Results: The files of 43 cases with second branchial cleft anomaly were examined. Of these, 39 (90.7%) were cysts and 4 (9.3%) were fistulas. The mean age was 24±13(3-66) years. The main complaint was swelling mass at the neck in all cases(100%). 4 (9.3%) had a history of infected cysts. The mean size of the cysts was 3.29±1.94(2-9.5) cm. Fine needle aspiration cytology(FNAC) was performed in 17 (39.53%) of the cases. Atypical cells- suspicion of malignancy was reported at FNAC of 4 (23.5%) cases, and of 13 cases (76.5%) were reported as benign. In our FNAC series, the false positives has a rate of 23.5%. As the most advanced imaging method, ultrasonography (USG), computed tomography(CT) and magnetic resonance imaging (MRI) were performed in 13 (30.3%), 11 (25.5%) and 19 (44.1%) cases respectively. USG only was performed as the most advanced imaging method in 50% of the patients in 2008, however in 2018, 3 (75%) of the cases were evaluated with MRI and 1 (25%) case was evaluated with CT. Surgical excision of the cyst or fistula tract excision under general anesthesia was performed for treatment in all cases. Surgical pathology was consistent with branchial cyst or fistula in all cases. Superficial skin infection occurred in 2 (4.6%) patients in the postoperative period. No recurrence was detected in the follow-up period (0%).
Conclusion: CT and MRI for imaging of second branchial cleft anomalies, and FNAC differentiation from other malignant cystic lesions has become more commonly used over the years. Surgical treatment is the treatment of choice for second branchial cleft anomalies. The complication and recurrence rates are very low with appropriate surgical excision.
Introduction
Branchial arches, embryological precursor of the ear and muscles, blood vessels, bones, cartilage and mucosal lining of face, neck and pharynx, develop between the fourth and seventh week of gestation. Altered development of these during embryogenesis may result in branchial anomalies such as cysts, fistulas, or islands of cartilages [1,2]. Branchial cysts account for 20% of cervical neck masses and 95% of these cysts originate from the second branchial arch [3]. First branchial cleft cysts consist of 1-4% of branchial cleft cysts, while third and fourth branchial cysts are extremely rare [3,4].The diagnosis of branchial cyst is based on clinical and radiological findings. The patient usually presents with painless, soft masses on the lateral aspect of the neck. It usually occurs unilaterally with no significant sex predilection [5]. Although branchial cysts exist from birth, they are usually detected between second and fourth decade of life [1]. They become symptomatic and enlarge after upper airway infection [6]. Ultrasonography (USG) is usually first line imaging method, however for further differential diagnosis computed tomography (CT) and/or magnetic resonance imaging (MRI) can be used [7]. The primary modality of treatment of branchial cyst is surgery [8,9]. Although they are benign, superinfection, mass effect and surgical treatment contribute to their morbidity. Fine needle aspiration cytology (FNAC) is sometimes used in the preoperative evaluation.
In this study, we aimed to evaluate clinical features of our second branchial cleft anomaly cases, review the diagnostic methods and the results of surgical treatment.
Methods
Patient files of second branchial cyst cases which were managed surgically between 2008 and 2018 in the Otolaryngology department of Haseki Training and Research Hospital were examined retrospectively. Patient characteristics such as age, gender, history of superinfection were noted. Presenting symptoms, preoperative investigations such as imaging and cytology, surgical pathology results, surgical complications were examined retrospectively. Recurrence rates, patient characteristics with recurrence and the treatment modalities used in them were compared with the cases which did not have recurrence. Institutional permission was obtained from the institutional review board (2018/293). No informed consent was obtained from patients because the study is a retrospective study. The study was conducted in accordance with the ethics principles laid down in the Helsinki Declaration.Results
The files of 43 patients with second branchial cleft anomaly were examined retrospectively. Of these, 39 (90.7%) were cysts and 4 (9.3%) were fistulas. The mean age of the patients was 24 ± 13 (3-66) years. Sixteen (37.2%) of the cases were male 27 (62.8%) were female (Table 1).){kind=link}
Table 1: Patient characteristics
The presenting symptom was swelling in the neck in all cases (100%). 4 (9.3%) had a history of infected cysts. 23 (53.48%) of the cases were on the right, 20 (46.52%) were on the left. The size of the cysts was 3.29 ± 1.94 (2-9.5) cm. Since between 2008-2010 years, fine needle aspiration cytology (FNAC) was not available in our institution no FNAC was performed. After its introduction, its use has increased and FNAC was performed in 75% of cases during the last two years in our series. In the whole series, FNAC was performed in 17 (39.53%) of the cases. Atypical cells- suspicion of malignancy was reported in 4 (23.5%) cases, and 13 cases (76.5%) were reported as benign. In our series, FNAC had a false positivity rate of 23.5%. Ultrasonography (USG), computed tomography (CT), and magnetic resonance imaging (MRI) were the most advanced imaging method performed in 13 (30.3%), 11 (25.5%) and 19 (44.1%) cases respectively. USG only was performed as the sole imaging method in 50% of the patients in 2008, however in 2018, 3 (75%) of the cases were evaluated with MRI and 1 (25%) case was evaluated with CT. Surgical excision of the cyst or fistula tract excision under general anesthesia was performed for treatment in all cases. Surgical pathology was consistent with branchial cyst or fistula in all cases. At the postoperative period, superficial skin infection occurred in 2 (4.6%) patients. The follow-up period was 16.11±6.95 (6-36) months. No recurrence was detected in the follow-up of the patients (0%).
Discussion
Branchial cleft cysts are developmental benign lesions arising from embryogenic branchial clefts. There are four types of branchial arch anomalies. Among them, the second branchial arch is the most common type and usually presents as a cyst [9,10]. Other branchial arch anomalies are less common than second branchial arch anomalies. All of patients included in this study had second branchial arch anomalies.Second branchial cleft cysts commonly present as lateral neck mass located anterior to sternocleidomastoid muscle between angle of mandible to the clavicle [8,9,11,12]. The patients usually present with painless swelling. Most of the cysts arise in patients between 20 to 40 years of age. However, there are reports in the literature with some branchial cleft cysts in infants and children younger than age of 5 [13]. The mean age of the patients was 24 ± 13 (3-66) years. There was no difference in localization and presentation of cysts in this study compared to previous studies but 7(16.28%) patients were in the pediatric age group and 2(4.6%) of them were under the age of five. Only 4 patients in our study had a history of infected cysts and were treated with antibiotherapy before surgery.
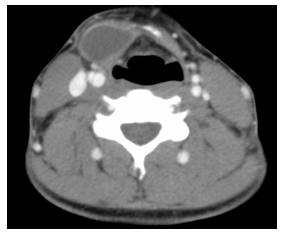
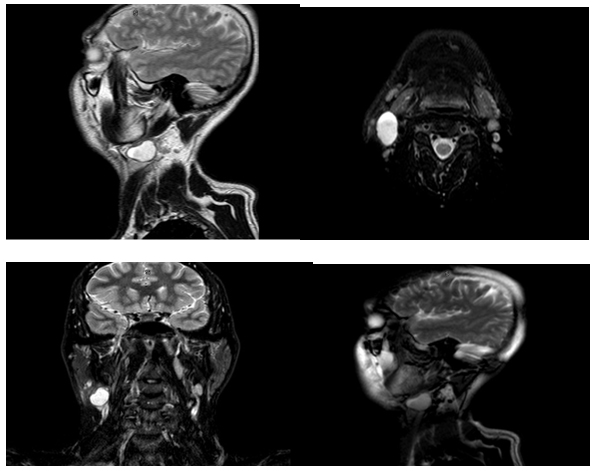
Diagnosis of branchial cleft cyst is usually based on history and physical examination. It is especially easy when a fistula is present at the skin [8,11,12]. However, there is no pathognomonic clinical or radiological findings of a branchial cleft cyst [4]. USG is usually the first line imaging method for neck masses as it is cheap and easy to perform. However, CT and MRI are preferred for identification of the relation of branchial cleft cyst with the surrounding important structures and differential diagnosis [4,8,9,11,14]. The displacement of sternocleidomastoid muscle, vessels of carotid space and submandibular gland can be seen on CT [15]. In the absence of infection, cysts are uniformly hypodense with a thin wall (Figure 1). Although MRI is more expensive, it provides more information about the depth of extension of the cyst. The cyst content appears as hypointense to isointense on T1-weighed sequences, and hiperintense on T2-weighed sequences [4,7,16] (Figure 2). Fistulography may be helpful to detect fistula tract [8]. As the most advanced imaging method, ultrasonography (USG), computed tomography(CT) and magnetic resonance imaging (MRI) were performed in 13 (30.3%), 11 (25.5%) and 19 (44.1%) cases respectively. USG only was performed as an imaging method 50% of the patients in 2008, however in 2018, 3 (75%) of the cases were evaluated with MRI and 1 (25%) case was evaluated with CT. We did not use fistulography in our 4 patients because cannulation is difficult and painful for the patient.
 Büyütmek İçin Tıklayın |
Figure 1: Computed tomographic image of a second branchial cleft cyst |
 Büyütmek İçin Tıklayın |
Figure 2: Image of a branchial brankial cyst in T1-weighed and T2-weighed Magnetic Resonance Imaging |
Metastatic squamous cell carcinoma, tuberculous lymphadenitis, HIV-related lymphadenitis, sarcoidosis, cat-scratch disease, lymphoma and metastatic papillary carcinoma of thyroid are included in the differential diagnosis of branchial cleft cysts [5,7,22]. Malignant components, such as bronchogenic carcinoma and papillary thyroid carcinoma have also been reported in the second branchial cyst setting [21]. However, no such cases were present in our case series.
In the preoperative evaluation of branchial cleft cysts, FNAC can be useful. With high true positive and true negative rates, FNAC is useful and simple technique for solid neck masses. However due to hypocellular content of cystic lesions and the low sensitivity of FNAC in diagnosis of cystic nodal metastasis of 33 -50 %, the use of FNAC in branchial cyst is controversial [17,18]. Typically, FNAC of branchial cleft cyst reveals pus-like fluid, keratinised anuclear cells, squamous epithelium and amorphous debris [19]. Lee at al. [13] used FNAC in 18 patients and found 100% sensitivity, 100% positive predictive value and 100% diagnostic accuracy in case of branchial cleft cysts. However, Begbie at al. [20] found sensitivity of FNAC as 75% in case of branchial cleft cyst and much less reliable. Since between 2008-2010 years, FNAC was not available in our institution, no FNAC was performed during this period. After its introduction, its use has increased and FNAC was performed in 75% of cases just during the last two years of our study period. FNAC was performed in 17 (39.53%) of the cases. Atypical cells- suspicion of malignancy was reported in 4 (23.5%) cases, and 13 cases (76.5%) were reported as benign. Surgical pathology revealed no associated malignancy in our second branchial cyst cases. In our series, FNAC for second branchial cysts had a false positivity rate of 23.5%.
The primary treatment of branchial arch anomalies is surgical excision through transverse cervical approach [7,8,9,11]. The timing of surgery depends on patient age, size of lesion and history of infection. In this study, surgical excision of the cyst or fistula tract excision under general anesthesia was performed for treatment. Recurrence rate is very low if excision is adequate [11]. In our series, superficial skin infection occurred in 2 (4.6%) patients in the postoperative period. No recurrence was detected in the follow-up of the patients (0%). Ethanol ablation has also been reported as an alternative treatment method for patients who refuse or are ineligible for a surgical procedure [23].
Declarations of interest: none
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors
Conclusion
CT and MRI for imaging of second branchial cleft anomalies, and FNAC for differentiation from other malignant cystic lesions has become more commonly used over the years. The complication and recurrence rates are very low with appropriate surgical excision. FNAC may be valuable in exclusion of malignant components of second branchial cleft cysts.Reference
1) Valentino M, Quiligotti C, Carone L. Branchial cleft cyst. J Ultrasound. 2013;16:17-20. [ Özet ]
2) Papadogeorgakis N, Petsinis V, Parara E, Papaspyrou K, Goutzanis L, Alexandridis C. Branchial cleft cysts in adults. Diagnostic procedures and treatment in a series of 18 cases. Oral Maxillofac Surg. 2009; 13: 79-85. [ Özet ]
3) Koeller K, Alamo L, Adair C, Smirniotopoulos J. Congenital cystic masses of the neck: radiologic-pathologic correlation.Radiographics. 1999; 19: 121-146. [ Özet ]
4) Adams A, Mankad K, Offiah C, Childs L. Branchial cleft anomalies: a pictorial review of embryological development and spectrum of imaging findings. Insights Imaging. 2016; 7: 69-76. [ Özet ]
5) Thomaidis V., Seretis K., Tamiolakis D., Papadopoulos N., Tsamis I. Branchial cysts. A report of 4 cases. Acta Dermatovenerol. Alp. Panonica Adriat. 2006; 15: 85-89. [ Özet ]
6) Muller S., Aiken A., Magliocca K., Chen A.Y. Second branchial cleft cyst. Head Neck Pathol. 2015; 9: 379-383. [ Özet ]
7) Bocchialini G., Bozzola A., Daleffe F., Ferrari L., Castellani A. Unusually rapid development of a lateral neck mass: Diagnosis and treatment of a branchial cleft cyst. A case report. Int J Surg Case Rep. 2017; 41: 383-386. [ Özet ]
8) Goff CJ, Allred C, Glade RS. Current management of congenital branchial cleft cysts, sinuses, and fistulae. Curr Opin Otolaryngol Head Neck Surg. 2012; 20: 533-539. [ Özet ]
9) Guldfred LA, Philipsen BB, Siim C. Branchial cleft anomalies: accuracy of pre-operative diagnosis, clinical presentation and management. J Laryngol Otol. 2012; 126: 598-604. [ Özet ]
10) Acierno SP, Waldhausen JH. Congenital cervical cysts, sinuses and fistulae. Otolaryngol Clin N Am. 2007; 40: 161-76. [ Özet ]
11) Prosser JD, Myer CM 3rd. Branchial cleft anomalies and thymic cysts. Otolaryngol Clin North Am 2015; 48: 1-14. [ Özet ]
12) Teng SE, Paul BC, Brumm JD, et al. Endoscope-assisted approach to excision of branchial cleft cysts. Laryngoscope. 2016; 126: 1339-1342. [ Özet ]
13) Lee DH, Yoon TM, Lee JK, Lim SC. Clinical Study of Second Branchial Cleft Anomalies. J Craniofac Surg. 2018; 29: e557-e560. [ Özet ]
14) Schroeder JW Jr, Mohyuddin N, Maddalozzo J. Branchial anomalies in the pediatric population. Otolaryngol Head Neck Surg 2007;137: 289-295. [ Özet ]
15) Mitroi M, Dumitrescu D, Simionescu C, Popescu C, Mogoanta C, Cioroianu L et al. Management of second branchial cleft anomalies. Rom J Morphol Embryol. 2008; 49: 69-74. [ Özet ]
16) Ibrahim M., Hammoud K., Maheshwari M., Pandya A.Congenital cystic lesions of the head and neck. Neuroimaging Clin. N. Am. 2011; 21: 621-639. [ Özet ]
17) Sheahan P, O"Leary G, Lee G, Fitzgibbon J. Cystic cervical metastases: incidence and diagnosis using fine needle aspiration biopsy. Otolaryngol Head Neck Surg. 2002; 127: 294-298. [ Özet ]
18) Rapidis AD, Faratzis G, Lagogiannis G, Koutsoubi K. Large swelling of the lateral neck. J Oral Maxillofac Surg. 2005; 63: 820-8. [ Özet ]
19) Valentino M., Quiligotti C., Carone L., Branchial cleft cyst, J. Ultrasound. 2016; 16: 17-20. [ Özet ]
20) Begbie F., Visvanathan V., Clark LJ. Fine needle aspiration cytology versus frozen section in branchial cleft cysts. J Laryngol Otol. 2015;129 :174-8. [ Özet ] Etit D, Yiğit S, Altindağ Sd, Ekinci N, Özkul Y, Çakalağaoğlu F, Brankial Kleft Kistleri: On Bir Yıllık Tek Merkez Serisi. Ege Klinikleri Tıp Dergisi. 2016; 54: 138-141.
21) Chen M.F., Ueng S.H., Jung S.M., Chen Y.L., Chang K.P. A type II first branchial cleft cyst masquerading as an infected parotid Warthin's tumor. Chang Gung Med. J. 2006; 29: 435-439. [ Özet ]
22) Ha EJ, Baek SM, Baek JH, Shin SY, Han M, Kim CH. Efficacy and Safety of Ethanol Ablation for Branchial Cleft Cysts. AJNR Am J Neuroradiol. 2017; 38: 2351-2356. [ Özet ]