


BPPV ATTACK WITH TWO LATENT PERIODS AND DURATIONS
2Medipol University Hospital, Sisli-Istanbul, Turkey
3Meydan Medical Center, Kulak Burun Boğaz, Antalya, Turkey
Summary
Posterior semicircular canal benign paroxysmal positional vertigo (P-SCC BPPV) presents a temporary vertigo and rotatory type nystagmus at the end of a latency period. There are two main hypotheses to explain the development of BPPV: cupulolithiasis and canalithiasis. In this case study we present a patient with two latent periods and two periods of nystagmus and elaborate on the reason for these phenomena.Introduction
Benign paroxysmal positional vertigo (BPPV) is the most common cause of dizziness and occurs as a result of head motion, leading to temporary vertigo. The most common semicircular canal involved in BPPV is the posterior semicircular canal (P-SCC) and is affected in approximately 87% of cases[1]. Dix and Hallpike[2] reported a maneuver to demonstrate the presence of temporary vertigo (5-30 seconds) at the end of a latency period. The presence of vertical up-beating and rotatory-type nystagmus toward the lower ear when the patient is laid down and nystagmus developing in the opposite direction, along with the occurrence of vertigo when brought back to a sitting position confirm the diagnosis. Resolution of vertigo and nystagmus is typical with resumption of the positioning maneuver[3]. As it is not possible to record the torsional component of this type of nystagmus by standard techniques, an electronystagmographic study is pointless.Temporary vertigo and nystagmus after a latent period are typical for BPPV and each show variation in duration. The latent period is usually observed to vary from a few seconds to 15 seconds[4,5]. In the following case we have portrayed a patient who underwent the Dix-Hallpike maneuver and after a short latency period displayed temporary vertigo with nystagmus and then after another short latency period showed another bout of temporary vertigo and nystagmus and we have discussed the probable mechanisms involved in these phenomena.
Case Presentation
A 49-year-old male had complaints of brief episodes of vertigo while looking up, bending forward or lying down that had been present for 20 days. Ear, nose, throat and neurologic examination results were all normal. The Dix-Hallpike test was performed on the patient while wearing Frenzel glasses and the process was video monitored. The right Dix-Hallpike maneuver resulted in vertical up-beating and torsional nystagmus toward the right ear and vertigo lasting for 14 seconds with a latency of 2 seconds. After cessation of vertigo and nystagmus another bout of vertigo and nystagmus lasting 15 seconds was observed after a 9 second latent period with the patient still in the supine position. When the patient returned to the sitting position, the direction of nystagmus was reversed. Another bout of vertigo and nystagmus lasting approximately 20 seconds after a 5 second latent period was observed during a repeat Dix-Hallpike maneuver. Fifteen minutes after the Dix-Hallpike test, the patient underwent the modified Epley canalith repositioning procedure (CRP). When the patient was placed in a supine position with the neck extended (Dix-Hallpike position) an attack of nystagmus and vertigo lasting 22 seconds was seen after a 5 second latent period. After having the patient stay for 1,5 minutes in this position, his head was rotated 90º toward the opposite side and the remaing sequence for the Epley procedure was completed . The patient was re-evaluated after 5 days and using the Dix-Hallpike test. No nystagmus or vertigo was seen during the test and the patient had no subjective complaints.Discussion
P-SCC is the most commonly involved canal in BPPV since the posterior canal is in the most gravity-dependent position. There are two main hypotheses to explain the development of BPPV; Schucknecht[6] proposed the cupulolithiasis theory, which is based on the attachment of otolithic debris to the cupula in the crista ampullaris. According to the cupulolithiasis theory, particles attached to the cupula enhance its weight and therefore cause aberrant deflection and stimulation during movement. In the second hypothesis, Hall et al.[7] propose the canalithiasis theory, which is based on the presence of free floating debris in the canal. With head movement, particles move in the endolymph with the help of gravity and thus cause abnormal displacement of the cupula resulting in aberrant neural stimulation. The cupula deflection ends when the clot reaches its lowest position in the canal[4].The phenomenon of the characteristic latency related to BPPV is explained by movement of detached otoconia through the ampulla. The latency relates to the fact that pressure caused by moving otoconia is negligible until otoconia enter the semicircular canal duct which is narrower hence creating a more powerful pull/push effect[8]. According to these hypotheses nystagmus and vertigo observed after a short latent period may be explained with the cupulolithiasis theory whereas longer latent periods may be rationalized by the canalithiasis theory.
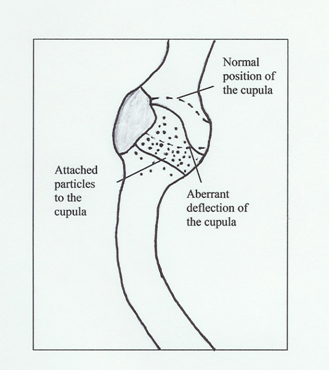
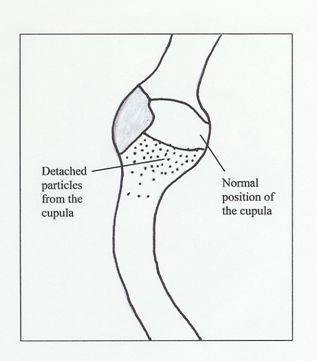
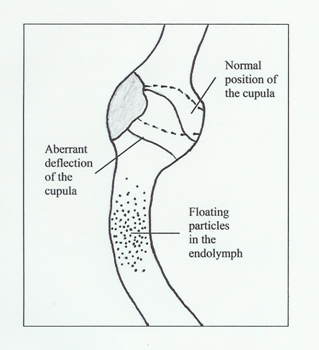
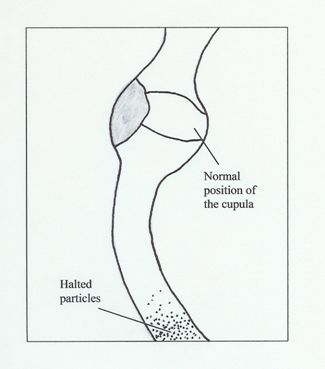
The presence of two different attacks of vertigo and nystagmus in our case during the Dix-Hallpike maneuver suggests that both the canalithiasis and cupulolithiasis theories may play a role in the mechanism of BPPV. We believe that the probable mechanism involved in our case is as follows: 1) When the patients' head was extended during the Dix-Hallpike maneuver, the first attack of vertigo and nystagmus after a 2 second latent period was initiated by the extensive deflection of the cupula caused by attached particles leading to exaggerated stimulation. 2) The return of the cupula to its normal position after detachment of the particles. 3) The clustering of the now free floating particles in the canal leading to a mass effect which in turn led to downward displacement of the cupula. 4) The relocation of the cupula to its normal position after the particles reached the end of the canal (Figure 1-4). Another possibility is that in our patient's case, there may have been free floating particles in the canal which may have clumped together with the particles that were detached from the cupula during the maneuver, resulting in a mass effect, thus leading to a second attack. One may wonder why 2 attacks with 2 latent periods is not a common phenomenon. A possible explanation is that particles detaching from the cupula do not have the ability to form the sufficient mass required to create an attack of nystagmus and vertigo[9]. Another reason may be that the stimulus caused by particle motion in the canal is masked by the first stimulus.
 Büyütmek İçin Tıklayın |
Figure 1: The exaggerated deflection of the cupula with attached particles 2 seconds after the initiation of the Dix-Hallpike maneuver leads to the onset of nystagmus and vertigo. |
 Büyütmek İçin Tıklayın |
Figure 2: The relocation of the cupula after detachment of its` particles and the cessation of nystagmus and vertigo after 14 seconds. |
 Büyütmek İçin Tıklayın |
Figure 3: The shift of the particles on the ampulla into the canal causing a mass affect which in turn causes downward displacement of the cupula resulting in aberrant deflection after 9 seconds. This leads to the second attack of nystagmus and vertigo. |
 Büyütmek İçin Tıklayın |
Figure 4: Particles coming to a resting position after reaching the lowest end of the canal and the return of the cupula to it's normal position after 15 seconds and the resolution of nystagmus and vertigo. |
As a result our case proves that both the cupulolithiasis and canalithiasis mechanisms can play a role in BPPV and both mechanisms may be seen in the same patient but further research is required.
Reference
1) Çakır BO, Ercan I, Çakır ZA, Civelek S, Sayın I, Turgut S. What is the true incidence of horizontal semicircular canal benign paroxysmal positional vertigo? Otolaryngol Head Neck Surg 2006;134:451-454. [ Özet ]
2) Dix MR, Hallpike CS. The pathology, symptomatology and diagnosis of certain common disorders of the vetibular system. Proc Soc Med 1952;45:341-354. [ Özet ]
3) Baloh RW, Sakala SM, Honrubia V. Benign paroxysmal positional nystagmus. Am J Otolaryngol 1979;1:1-6 [ Özet ]
4) Korres SG, Balatsouras DG. Diagnostic, pathophysiologic, and therapeutic aspects of benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg 2004;131:438-444. [ Özet ]
5) Bourgeois PM, Dehaene I. Benign paroxysmal positional vertigo (BPPV): clinical features in 34 cases and review of literature. Acta Neurol Belg 1988;88:65-74. [ Özet ]
6) Schuknecht HF. Cupulolithiasis. Arch Otolaryngol 1969;90:765-778. [ Özet ]
7) Hall SF, Ruby RRF, McClure JA. The mechanics of benign paroxysmal positional vertigo. J Otolaryngol 1979;8:151-158. [ Özet ]
8) Hain TC, Squires TM, Stone HA. Clinical implications of a mathematical model of benign paroxysmal positional vertigo. Ann N Y Acad Sci 2005;1039:384-394. [ Özet ]
9) Çakır BO, Ercan I, Çakır ZA, Civelek Ş, Turgut S. Relationship between the affected ear in benign paroxysmal positional vertigo and habitual head-lying side during bed rest. J Laryngol Otol 2006; [ Özet ]