


RECURRENT VOCAL CORD PARALYSIS ASSOCIATED WITH RIGHT AORTIC ARCH
2GATA, RADYOLOJİ, ANKARA, Türkiye
Summary
We report the first case of right recurrent vocal cord paralysis associated with right aortic arch. A 37-years old male presented with progressive hoarseness of voice that has begun within the last six weeks. He had a history of recurrent vocal cord paralysis occurring one and two years ago that last two and five months respectively. Fiberoptic laryngoscopy showed right vocal cord paralysis in a paramedian position. Chest CT scan revealed a right-sided aortic arch. It was believed that right-sided aortic arch was responsible for the compression of the right recurrent laryngeal nerve and right vocal cord paralysis.We report a recurrent vocal cord paralysis associated with right aortic arch which has never been reported in literature. This case may also be accepted as a different cause of cardiovocal syndrome.Introduction
Unilateral vocal cord paralysis is a disorder caused by dysfunction of the recurrent laryngeal or vagus nerve innervating the muscles of larynx. Vocal cord paralysis sometimes is the only or first symptom of an underlying disease. Thus, it is important to diagnose the primary disease underlying.[1] Vocal cord paralysis can be associated with malignancies (lung, thyroid), idiopathic reasons, post viral syndromes, iatrogenic reasons (thyroidectomy, intubation etc.), inflammatory diseases, trauma, neurogenic and neuromuscular diseases and cardiac diseases.[2-4] Vocal cord paralysis associated with cardiovascular system is termed as cardiovocal syndrome which is first reported in three mitral stenosis patients by Ortner.[2,3,5,6]Right aortic arch is a generally asymptomatic congenital anomaly that is seen in approximately %0.1 of the population.[7-12] It may be responsible for symptoms resulting from compression of either the trachea or the esophagus. Dysphagia, dyspnea and dysphonia are often reported symptoms in literature. Dysphonia and dyspnea are almost always reported due to relevant stenosis of the tracheal lumen compressed by aortic anomalies.[8,10-14] Vocal cord paralysis associated with right aortic arch has never been reported.
We report the first case of right recurrent vocal cord paralysis associated with right aortic arch in literature. Also, this case could be accepted as a different cause of cardiovocal syndrome.
Case Presentation
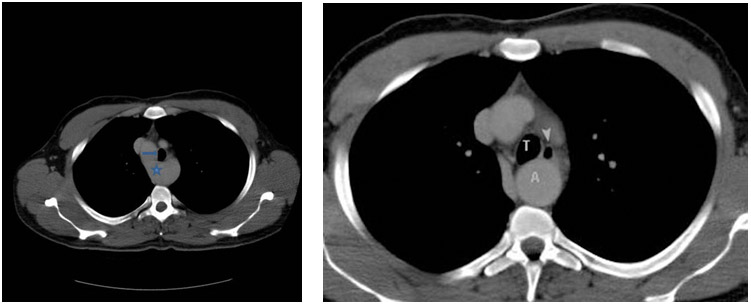
A 37-years old male presented with progressive hoarseness of voice that has begun within the last six weeks. He had a history of recurrent vocal cord paralysis occurring one and two years ago that last two and five months respectively. He was with normal general health and no other personal history of disease or smoking. Fiberoptic laryngoscopy showed right vocal cord paralysis in a paramedian position. There was no palpable mass in head and neck examination. Pulse and blood pressure were normal. Neurological examination was normal and there was no other cranial nerve abnormality. Tiroid ultrasonography was normal. A battery of Computed Tomography (CT) studies that include brain, neck and chest were performed. There were no significant findings related to paralysis in neck CT study. The brain CT scan was normal. Chest CT scan revealed a right-sided aortic arch. (Figure 1a, 1b) There was no mediastinal mass or enlarged lymph node and it was believed that right-sided aortic arch was responsible for the compression of the right recurrent laryngeal nerve and right vocal cord paralysis. The patient underwent cardiologic examination for other probable cardiac anomalies which could be associated with right aortic arch. Cardiologic examination including echocardiography was normal. The patient had no dysphagia, dyspnea and aspiration complaints. He had a transcutaneous injection laryngoplasty with fiberoptic trans-nasal guidance under local anesthesia to improve the voice quality. Patient was followed for spontaneous recovery. Five months later flexible endoscopic examination of the larynx showed complete remobilization of right vocal cord.
 Büyütmek İçin Tıklayın |
Figure 1: (a) Axial contrast-enhanced CT through upper mediastinum shows right aortic arch (star) causing a slight tracheal displacement (arrow). This site may be responsible for compression of right recurrent laryngeal nerve. (b) Axial contrast-enhanced CT at a lower level than (a) shows a slight anterior displacement of tracheal and esophageal structures due to distal portion of right aortic arch. T: Trachea, A: Distal portion of the right aortic arch, Arrowhead: Esophagus |
Discussion
The recurrent laryngeal nerve paralysis causes the vocal cord paralysis which generally presents with a characteristic breathy and/or hoarse voice often accompanied by swallowing disability, a weak cough, and the sensation of shortness of breath. The left recurrent laryngeal nerve arises from the left vagus at the level of the aortic arch, then hooks back posteriorly under the arch and ascends through the superior mediastinum to reach the groove between the trachea and esophagus. On the right side, the recurrent laryngeal nerve arises from the vagus nerve anterior to the subclavian artery then loops back under the artery and ascends posterior to the artery in the groove between the trachea and esophagus.[4] The function of the recurrent laryngeal nerve can be disrupted by pressure or by injury of the nerve along this pathway. Left recurrent laryngeal nerve is more vulnerable than right because it pursues a longer intrathoracic course, coming into contact with the mediastinal surface of the left lung, continuing along the mediastinal lymph nodes, and finally looping around the aortic arch.[1,15] In contrast to the normal, the aortic arch was right sided and vocal cord paralysis was on the right side in this case. The anatomic variation of this case may make right recurrent laryngeal nerve more vulnerable instead of left recurrent laryngeal nerve and be responsible of right vocal cord paralysis by compressing the right recurrent laryngeal nerve between arch and trachea. The history of recurrence on the same side and no other disease which could be related with vocal cord paralysis, are supportive of this.In the etiology of vocal cord paralysis, there are malignancies (lung, thyroid, skull base etc.), idiopathic reasons, post viral syndromes, iatrogenic reasons (thyroidectomy, carotid endarterectomy, intubation etc.), inflammatory diseases (thyroiditis, lyme disease), trauma, neurogenic and neuromuscular diseases (myasthenia gravis, spinocerebellar atrophy etc.) and cardiac diseases.[2-4] The recurrent laryngeal nerve paralysis associated with cardiovascular system is named as cardiovocal syndrome (Ortner's syndrome) which is first reported in 3 patients with mitral stenosis by ortner.[2,3,5,6] The pathology of the cardiovocal syndrome generally includes vascular dilatation and compression to the recurrent laryngeal nerve in the thorax, which has limited space due to a primary (aneurysm) or seconder (cardiac anomalies) diseases.[4,5,16] Although there are many cases in the literature about the cardiovocal syndrome, we could not find a vocal cord paralysis case associated with the right aortic arch without any other cardiac anomalies. Also, we have seen that aortic arch anomalies haven't been mentioned in the etiology of cardiovocal syndrome. Furthermore, cardiovocal syndrome is generally described for left recurrent laryngeal nerve but in this case vocal cord paralysis was on the right side. This may be due to the nature of right side localization of aortic arch. This case may be accepted as a different cause of cardiovocal syndrome.
Right aortic arch is a generally asymptomatic congenital anomaly that is seen in approximately %0.1 of the population.[7-12] Although, a variety of patterns of branching of the brachiocephalic vessels are seen in the context of a right aortic arch, there are two basic most characteristic sequences. First one of these is the origin of the brachiocephalic vessels from the arch in a mirror-image fashion. In this pattern first branch is left innominate artery followed by right common carotid artery and right subclavian artery successfully. The second typical branching pattern contains left common carotid artery as the first branch, followed by the right common carotid and subclavian arteries, then an aberrant left subclavian artery from the descending aorta via a diverticulum.[11] This case had a right aortic arch with mirror image-branching. The right aortic arch with mirror-image branching almost invariably accompanied by a congenital cardiac anomaly which is typically consist of Fallot tetralogy with or without pulmonary atresia, or truncus arteriosus. A right aortic arch with mirror-image branching and no concomitant cardiac abnormalities is extremely unusual.[11] This case didn't have a concomitant cardiac abnormality. Aortic arch anomalies may be responsible for symptoms resulting from compression of either the trachea or the esophagus. Dysphagia, dyspnea and dysphonia are often reported symptoms in literature. Dysphonia and dyspnea are almost always reported due to relevant stenosis of the tracheal lumen compressed by aortic anomalies.[8,10-14] This case had a symptom of dysphonia but no dysphagia and dyspnea. Although there was a slight displacement on trachea, contrast to the literature, in this case dysphonia was not associated with compressed tracheal lumen but recurrent laryngeal nerve paralysis which is caused by right aortic arch. Vocal cord paralysis associated with right aortic arch has never been reported in literature.
Conclusion
We report a recurrent vocal cord paralysis associated with right aortic arch which has never been reported in literature. This case may also be accepted as a different cause of cardiovocal syndrome. Cardiovascular abnormalities should always be kept in mind in the diagnosis of vocal cord paralysis.Reference
1) Song SW, Jun BC, Cho KJ, Lee S, Kim YJ, Park SH. CT evaluation of vocal cord paralysis due to thoracic diseases: a 10-year retrospective study. Yonsei Med J. 2011 Sep;52(5):831-7. [ Özet ]
2) Annema JT, Brahim JJ, Rabe KF. A rare cause of Ortner's syndrome (cardiovocal hoarseness). Thorax. 2004 Jul;59(7):636. [ Özet ]
3) Zaki SA, Asif S, Shanbag P. Ortner syndrome in infants. Indian Pediatr. 2010 Apr;47(4):351-3. [ Özet ]
4) Grundfast KM, Harley E. Vocal cord paralysis. Otolaryngol Clin North Am. 1989 Jun;22(3):569-97. [ Özet ]
5) Mulpuru SK, Vasavada BC, Punukollu GK, Patel AG. Cardiovocal Syndrome: A Systematic Review. Heart Lung Circ. 2008 Feb;17(1):1-4. Epub 2007 Dec 4. [ Özet ]
6) Plastiras SC, Pamboucas C, Zafiriou T, Lazaris N, Toumanidis S. Ortner's syndrome: a multifactorial cardiovocal syndrome. Clin Cardiol. 2010 Jun;33(6):E99-100. [ Özet ]
7) Ballotta E, Mion E, Bardini R. Right-sided aortic arch and aberrant left subclavian artery. J Cardiovasc Surg (Torino). 2003 Dec;44(6):783-4. [ Özet ]
8) Edwards JE. Anomalies of the derivatives of the aortic arch system. Med Clin North Am. 1948 Jul;32:925-49. [ Özet ]
9) Shuford WH, Sybers RG, Edwards FK. The three types of right aortic arch. Am J Roentgenol Radium Ther Nucl Med. 1970 May;109(1):67-74. [ Özet ]
10) Knight L, Edwards JE. Right aortic arch. Types and associated cardiac anomalies. Circulation. 1974 Nov;50(5):1047-51. [ Özet ]
11) McElhinney DB, Hoydu AK, Gaynor JW, Spray TL, Goldmuntz E, Weinberg PM. Patterns of right aortic arch and mirror-image branching of the brachiocephalic vessels without associated anomalies. Pediatr Cardiol. 2001 Jul-Aug;22(4):285-91. [ Özet ]
12) Tschirch E, Chaoui R, Wauer RR, Schneider M, Rüdiger M. Perinatal management of right aortic arch with aberrant left subclavian artery associated with critical stenosis of the subclavian artery in a newborn. Ultrasound Obstet Gynecol. 2005 Mar;25(3):296-8. [ Özet ]
13) Gross RE. Arterial malformations which cause compression of the trachea or esophagus. Circulation. 1955 Jan;11(1):124-34. [ Özet ]
14) Backer CL, Ilbawi MN, Idriss FS, DeLeon SY. Vascular anomalies causing tracheoesophageal compression. Review of experience in children. J Thorac Cardiovasc Surg. 1989 May;97(5):725-3. [ Özet ]
15) Titche LL. Causes of recurrent laryngeal nerve paralysis. Arch Otolaryngol. 1976 May;102(5):259-61. [ Özet ]
16) Nakahira M, Nakatani H, Takeda T. Left vocal cord paralysis associated with long-standing patent ductus arteriosus. AJNR Am J Neuroradiol. 2001 Apr;22(4):759-61. [ Özet ]