


RUPTURED PEXY AFTER SUPRACRICOID PARTIAL LARYNGECTOMY: A CASE REPORT
Summary
Background: The postoperative complication rate after supracricoid partial laryngectomy (SCPL) is low and comparable to those of other partial laryngectomy techniques. Rupture of the pexy after SCPL is rare and has been mentioned in the literature for three times.Methods: We present a case with ruptured pexy due to nonossified cricoid cartilage. Revision of the pexis was performed with resection of the transected anterior cricoid arch. Results. The patient was decannulated 35 days after revision surgery. The nasogastric feeding tube was removed in the 7th postoperative day.
Conclusion: It is important to consider the presence of a non-ossified cricoid cartilage and perform the tracheotomy on the 4th-5th tracheal rings in order to prevent the rupture of the pexy after SCPL. In case of the pexy rupture, releasing the epiglottis downwards during the revision surgery facilitates decannulation. If the surgeon does not consider the mentioned points, performing a total laryngectomy may be unavoidable.
Introduction
Supracricoid partial laryngectomy (SCPL) with cricohyoidopexy and cricohyoidoepiglottopexy, introduced in 1959 and 1974, respectively, has rapidly demonstrated its functional and oncologic efficiency for the treatment of selected glottic, supraglottic and transglottic cancers [1,2].Cases with suspected invasion of the hyoid bone or the cricoid cartilage, fixation of the cricoarytenoid joint, massive pre-epiglottic space invasion, posterior commisure involvement or extralaryngeal tumor invasion were not proposed for SCPL. Patients with systemic involvement (such as chronic pulmonary disease, uncontrolled diabetes mellitus or cardiovascular disorders) or intellectually unable to attain deglutition rehabilitation courses were not considered eligible for this type of surgery [2,3].
Complications after SCPL have been established as a wound infection, hematoma, postoperative bleeding, pneumonia due to aspiration, laryngeal necrosis, laryngeal stenosis, bilateral or unilateral arytenoid immobility and retro-cricoid ulceration from nasogastric feeding tube in the literature [2,4]. First three complications were statistically related only to neck dissection. Ruptured pexy after SCPL is a rare event [5]. In this paper we presented and discussed a case with ruptured pexy following SCPL.
Case Presentation
A 57-year-old man with glottic carcinoma and impaired motion of true vocal cord staged as T2N0M0 according to the American Joint Committee on cancer classification system. 6 underwent SCPL-cricohyoidoepiglottopexy sparing two arytenoid cartilages. He had a controlled diabetes mellitus. The patient was noted to have an elevated skin flap over tracheostoma, aspiration, and revealed a gap between the hyoid bone and the cricoid cartilage by the 5th postoperative day. The patient was taken into the operating room and it was noted that the pexy sutures had cut through the anterior arch of the cricoid cartilage (Figure 1, 2). Revision of the pexis was performed with resection of the transected anterior cricoid arch. The epiglottis was released downwards until the level of the anterior cricoid arch. The trachea was sutured to the hyoid bone by means of the circular sutures with three submucosal 1 Vicryl sutures looped around the trachea, passed through the epiglottic cartilage, then passed back into the preepiglottic fat, looped around the hyoid bone, and then passed deep into the tongue base (Figure 3). The postoperative course was unremarkable. The nasogastric feeding tube was removed 7 days after revision surgery. The patient was decannulated 35 days after revision surgery.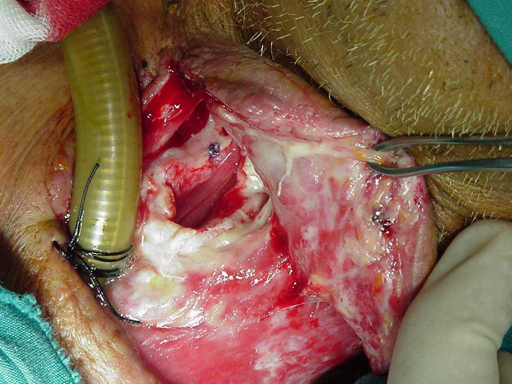 | Ruptured pexis. Note the 4-cm gap between upper edge of the cricoid cartilage and the hyoid bone. |
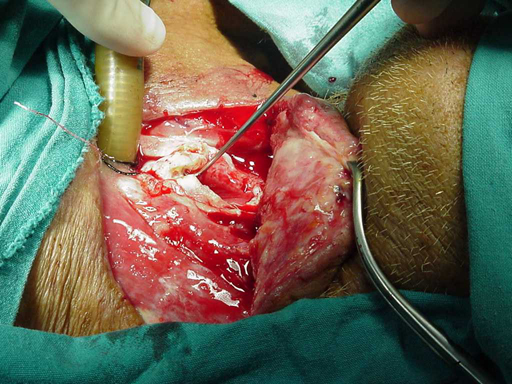 | The instrument points the transected cricoid arch that will be resected. |
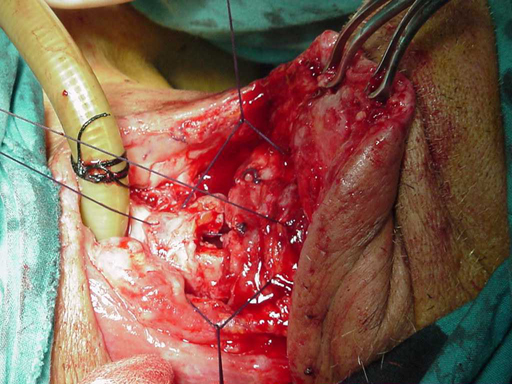 | Tracheocricohyoidoepiglottopexy sutures for re-reconstruction. |
Discussion
SCPL allowed a reduction of the indications for total laryngectomy in advanced endolaryngeal carcinomas [1,4]. Twenty-six SCPL were performed in our department between January 1994 and October 2001. One patient had separation between the hyoid bone and the cricoid cartilage due to a ruptured pexy in the postoperative period 0.04%).The complication rate after SCPL is low and comparable to that of other vertical or horizontal partial laryngectomy techniques [2,5]. Ruptured pexy is rare but severe complication after SCPL. This complication has been mentioned for three times in the literature [2,5,7] and its incidence is reported as 0.8% [5]. Ruptured pexy must be systematically excluded when major aspiration is noted during the immediate postoperative period or in case of chronic aspiration later [2]. If palpation of the anterior part of the neck demonstrates a gap between the hyoid bone and the cricoid cartilage with the presence of the massive aspiration, then a ruptured pexy should be suspected. Lateral cervical radiography or computerized tomography is recommended for the evaluation of the distance between the hyoid bone and the cricoid cartilage [2,5,7]. Early rupture of the pexy was related to partial resection of the cricoid arch, cricoid trauma due to emergency recannulation, presence of a nonossified cricoid cartilage, and tension on the sutures between the cricoid cartilage and the hyoid bone. Delayed pexy rupture can occur and is due to a progressive separation between the cricoid cartilage and hyoid bone [2]. We found out that the rupture of the pexy was due to transection of the cricoid arch due to sutures. To avoid this complication, dissection of the mediastinal trachea up to the carina during the operation may be useful especially in patients with non-ossified cricoid cartilages. This maneuver allows upward mobility of the trachea at the time of closure and eliminates tension at the suture line [2,5,8]. Patients in whom the cricoid cartilage is not ossified or the anterior arch is resected due to tumor extension, the first tracheal ring should be looped submucosally [2,5,8]. We revised the SCPL by means of the tracheocricohyoidopexy after resection of the transected anterior cricoid arch with three no:1 Vicryl sutures (Figure 3). More sutures will flatten the tongue and reduce its efficiency at the time of swallowing. 1 Performing the tracheotomy at the level of 4th-5th tracheal rings is also important to re-suture the ruptured pexy. In the case of an upper tracheotomy site, repair of a ruptured pexy may be impossible.
We used to remove the tracheotomy tube before the nasogastric feeding tube after SCPL. In this patient, we removed the nasogastric feeding tube before the closure of the tracheotomy site. We started the swallowing exercise just after the revision surgery and the patient could eat and drink without aspiration 7 days after the revision. Although we tried decannulation several times after surgery (first attempt was on postoperative 5th day), we could manage it by the postoperative 35th day.
In our opinion, ruptured pexy is a repairable complication and should not lead to total laryngectomy prior to an attempt of re-suturing the pexy.
Reference
1) Laccourreye H, Laccourreye O, Weinstein G, Menard M, Brasnu D. Supracricoid partial laryngectomy with cricohyoidopexy: a partial laryngeal procedure for selected supraglottic and transglottic carcinomas. Laryngoscope 1990; 100:735-741. [ Özet ]
2) Brasnu DF, Hartl DM, Laccourreye H. Supracricoid partial laryngectomy with cricohyoidopexy. In: Weinstein G, editor. Organ preservation surgery of laryngeal cancer. San Diego ,CA: Singular publishing. 2000;127-148.
3) Ferlito A, Silver CE, Howard DJ, Laccourreye O, Rinaldo A, Owen R. The role of partial laryngeal resection in current management of laryngeal cancer: a collective review. Acta Otolaryngol 2000; 120:456-465. [ Özet ]
4) Naudo P, Laccourreye O, Weinstein G, Jouffre V, Laccourreye H, Brasnu D. Functional outcome and prognosis factors after supracricoid partial laryngectomy with cricohyoidopexy.Ann Otol Rhinol Laryngol1997;06:291-296. [ Özet ]
5) Laccourreye O, Brasnu D, Laccourreye L, Weinstein G. Ruptured pexis after supracricoid partial laryngectomy. Ann Otol Rhinol Laryngol 1997;106:59-162. [ Özet ]
6) Beahrs OH, Henson DE, Hutter RVP, Myers M, eds. American Joint Committee on Cancers. 3rd ed. Philadelphia : JB Lippincott. 1998;39-44.
7) Traissac L, Verhulst J. Indications, tecniques et resultats des laryngectomies reconstructives . Rev Laryngol Otol Rhinol (Bord) 1991;112:55-58. [ Özet ]
8) Laccourreye O, Ross J, Brasnu D, Chabardes E, Kelly JH, Laccourreye H. Extended supracricoid partial laryngectomy with tracheo cricohyoido epiglottpexy. Acta Otolaryngol (Stockh) 1997;114:669-674. [ Özet ]