


CAVERNOUS HEMANGIOMA OF MAXILLARY SINUS IN AN ADULT MIMICKING CARCINOMA
2Karadeniz Technical University Faculty of Medicine, Department of Pathology, Trabzon, Turkey
Introduction
Hemangiomas are common lesions of the head and neck, which predominantly originate from lips, tongue and buccal mucosa [1]. However; sinonasal hemangiomas are rare and when they occur they usually arise from nasal septum and vestibule [2]. Being rare, they can cause diagnostic and therapeutic problems. We report a cavernous maxillary sinus hemangioma in a 65 -year-old male causing medial maxillary wall destruction and mimicking malignancy.Case Presentation
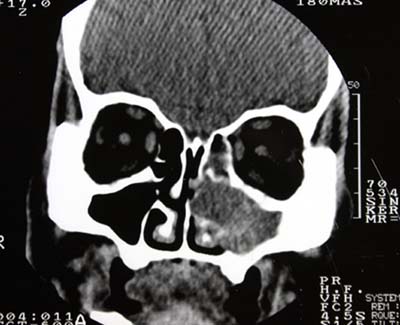
A 65 year-old male patient was admitted to our department with complaints of recurrent abundant epistaxis, progressive nasal obstruction at the left side and a sensation of fullness at his left cheek for 2 months. In anterior rhinoscopy, a mass originating from left nasal wall was obstructing the passage. Endoscopy showed that the mass was hard in nature and almost completely blocked nasal passage. There was no purulent or mucous secretion present. Computerized tomography (CT) revealed a soft tissue mass in the left maxillary sinus expanding the lateral nasal wall medially with accompanying bone destruction (Figure 1). A preoperative diagnosis of malignancy could not be ruled out with respect to the histopathology report which mentioned the presence the tortuous dilated blood vessels accompanied with scanty atypical cells. Medial maxillectomy was performed via a lateral rhinotomy incision. A red-purple colored, soft and fragile mass was excised en bloc with lateral nasal wall and inferior turbinate. Polypoid tissues originating from anterior ethmoidal cells and anterior of the middle turbinate were also resected. There was no significant bleeding during the surgery and the tumor was easily removed. Histopathology reported a cavernous hemangioma (Figure 2). The patient made a complete recovery. In the four-year follow up period no evidence of recurrence was observed.
 Büyütmek İçin Tıklayın |
Figure 1: Computerized tomography (CT) revealed a soft tissue mass in the left maxillary sinus expanding the lateral nasal wall medially with accompanying bone destruction. |
 Büyütmek İçin Tıklayın |
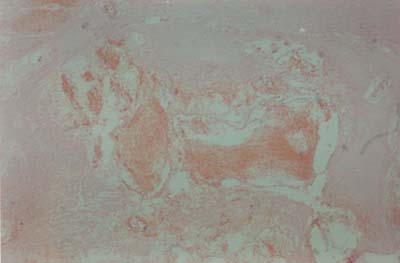
Figure 2: Histopathological section demonstrating cavernous hemangioma (Hematoxylin-eosin stained under 400 magnification) |
Discussion
Hemangiomas are usually classified into three categories; capillary, cavernous and combined (capillary-cavernous). The dominant vessel size at microscopy determines the type of a hemangioma [3]. Capillary hemangiomas are the most common vascular lesions and microscopically they appear as dense masses of epithelial cells with multiple capillary channels. Cavernous hemangiomas have a microscopic appearance of large blood-filled canals lined with a single layer of endothelial cells and separated by scant connective tissue stroma. Histologically they are sharply defined but encapsulated lesions. Nasal septum and the vestibule are the most common sites of sinonasal hemangiomas, which are predominantly cavernous type [2]. Maxillary sinus hemangiomas are extremely rare [4]. A recent review reported only 17 maxillary sinus hemangioma cases in the literature [5].Maxillary sinus hemangiomas grow slowly and causes local destruction due to pressure effect [6]. The major symptoms are recurrent epistaxis and nose obstruction, whereas gradual swelling of the face, sinus headaches and loosing of the maxillary teeth may also be seen. In imaging studies they appear as non-homogeneous masses [2]. Pooling of the blood in the mass and the presence of necrotic areas are held responsible for this non-homogeneity. They typically give rise to changes in adjacent bone and gradually expansion of the sinus develops [2]. Bone destruction, which is easily misinterpreted as a sign of malignancy may also accompany these findings [3]. In addition, they may contain phleboliths due to dystrophic calcification following intravascular thrombosis. Differential diagnosis should include neuroma, inverted papilloma, mucocele, and other benign or malignant vascular tumors [6]. The imaging modalities of choice are CT and MRI, however none of these provide pathognomonic data for hemangiomas [6]. They are especially of use to reveal the boundaries and the soft tissue extension of the lesion.
In our case, medial displacement of the medial maxillary sinus wall showed that the mass was originating within the maxillary sinus (Figure 1). Although there were areas of remodeled bone, destruction of the lateral nasal wall was considered as a sign of malignancy. The opacification in the anterior and middle ethmoidal cells were interpreted as inflammatory disease secondary to obstruction of the middle meatus, which was later proved to be true in the surgery.
Intraoperative hemorrhage related to hemangiomas is variable and may present with minimal or massive bleeding [5]. Since surgical intervention of hemangiomas can lead to severe blood loss, when a vascular tumor is suspected in the preoperative diagnosis, angiography and if necessary transarterial embolization of the feeding vessels should be considered. Complete excision of the tumor is the treatment of choice and no recurrence has been reported following paranasal hemangioma surgery.
Reference
1) Most DS. Hemangioma of the maxillary sinus. Oral Surg Oral Med Oral Pathol 1985; 60: 485-486. [ Özet ]
2) Kim HJ, Kim JH, Kim JH, Hwang EG. Bone erosion caused by sinonasal cavernous hemangioma: CT findings in two patients. AJNR Am. J. Neuroradiol. 1995; 16: 1176-1178. [ Özet ]
3) Dillon WP, Som PM, Rosenau W. Hemangioma of the nasal vault: MR and CT features. Radiology 1991;180: 761-765. [ Özet ]
4) Starska K, Lukomski M, Danilewicz M. Hemangioma cavernous of the nasal cavity and the maxilary sinus-case report and review of the literature. Otolaryngol Pol 2006;60(6): 955-7. [ Özet ].
5) Harar RP, Wolfe KQ, Kumar S, Gatland DJ. Haemangioma of the frontal sinus. J. Laryngol. Otol. 2002;116: 296-298. [ Özet ].
6) Jammal H, Barakat F, Hadi U. Maxillary cavernous hemangioma: a rare entity. Acta Otolaryngol 2004; 124(3):331-333. [ Özet ].