


NASAL SEPTAL PAPILLOMA CO-EXISTING WITH A RHINOLITH: CASE REPORT
Summary
Nasal septal papillomas are rare benign epithelial neoplasms with obscure etiology. In this report, an exophytic nasal septal papilloma co-existing with a rhinolith is presented in a 17-year-old male patient, whose complaints were unilateral nasal stuffiness and discharge. On examination, a papillomatous mass occluding right nasal passage was observed. Open-technique septorhinoplasty, excision of papilloma and extraction of the rhinolith was performed simultaneously and the patient's complaints were relieved afterwards. Even though there is not sufficient supportive data in the literature, the co-existence of a rhinolith and a nasal septal papillomas made us think that these two entites may be inducing the formation of each other.Introduction
Nasal septal papillomas are benign, polypoid lesions that exist infrequently. They mostly occur unilaterally and are composed of well-differentiated columnar or ciliated respiratory epithelium with variable squamous differentiation[1].Foreign bodies in the nose are usually seen in children and debilitated patients. Non-living foreign bodies, either endogenous or exogenous, may present as rhinoliths[2]. Rhinoliths are composed of calcium and magnesium phosphate, oxalate and carbonate salts, which priorly accumulate around an organic or inorganic nidus in the beginning. The most common symptoms of a rhinolith are unilateral nasal stuffiness, foul-smelling, bloody or purulent discharge, and headache secondary to sinusitis [2,3].
As far as we know, a nasal septal papilloma co-existing with a rhinolith has not been reported up to now. Even though, the literaure lacks sufficient data on the co-existence of these two “separate” issues and a definitive etiologic relationship; a nasal papilloma and a rhinolith may have an inducive effect on the formation of each other.
Case Presentation
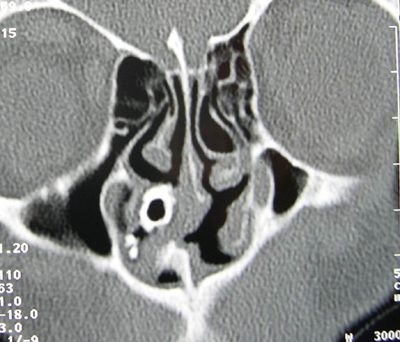
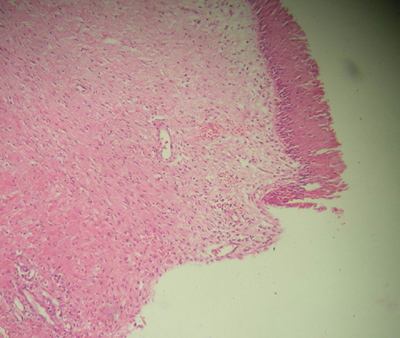
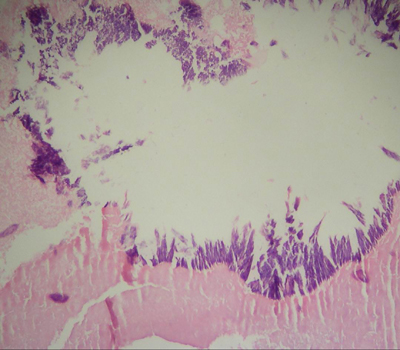
A 17-year-old male patient, who had been complaining of nasal stuffiness, foul-smelling discharge and a mass protruding out of right nostril on forced expiration, applied to our clinic. Anterior rhinoscopy revealed a prominent septal deviation towards left and a mass in posterior part of right nasal cavity. Paranasal sinus computerized tomography (CT) scans confirmed the septal deviation as well as the right nasal rhinolith (Figure 1). Under general anesthesia, the patient underwent an open-technique septorhinoplasty due to prominent nasal septal deformity and nasal hump. A papillomatous mass of 3X2X1 cm was encountered on right side of nasal septum. Behind the papilloma, a rhinolith was observed and excision of the papilloma was conducted together with the removal of the rhinolith (Figure 2). Histopathological examination of the biopsy specimens was reported as an exophytic nasal papillloma, and a calcified rhinolith (Figures 3, 4).
 Büyütmek İçin Tıklayın |
Figure 1: The preoperative CT scan demonstrating the right nasal septal papilloma and the rhinolith occluding the inferior meatus. |
 Büyütmek İçin Tıklayın |
Figure 2: The macroscopic view of nasal septal papilloma (right) and rhinolith (left) just after excision. |
 Büyütmek İçin Tıklayın |
Figure 3: The histopathologic section of the nasal septal papilloma with its villi (right, up) (HEX100). |
 Büyütmek İçin Tıklayın |
Figure 4: The histopathologic section of the rhinolith after the decalcification process (HEX100). |
Discussion
Rhinoliths may be formed due to an object lodged in the nasal cavity and calcified afterwards. The core of a rhinolith may be formed by seeds, buttons, beads, fragments of teeth etc. Rhinoliths mostly occur unilaterally and its chief symptoms are nasal obstruction, pain and foul smell. Their size may increase owing to precipitation of salts and ongoing mineralization on its surface [3]. A rhinolith existing for a long time tends to cause erosion of septum between nasal fossa and maxillary sinus, as well as resulting in the formation of bony or cartilaginous sequestrum [3]. Such a lesion may even give the impression of a osteogenic sarcoma or cause palatal perforation [4,5]. To our knowledge, their co-existence with nasal septal papillomas or any other benign or malignant neoplasia have not been reported in the literature up to now [3].Nasal papillomas are benign epithelial tumors that originate from the columnar or ciliated epithelium lining the nasal cavity. World Health Organization (WHO) had classified these tumors into 3 histopathological subgroups: 1. exophytic papilloma, 2. inverted papilloma, 3. columnar cell papilloma. Exophytic papillomas mainly originate from nasal septum, while inverted and columnar cell papillomas arise from lateral nasal wall or within the maxillary sinus. Sinonasal papillomas have a local expansive growth potential. Malignant transformation is very rare for exophytic papillomas, but it is reported to be 5-15% for inverted and columnar cell papillomas. Surgical intervention alone or surgery combined with radiotherapy constitute the alternatives for treatment of papilloma. Both external and endonasal approaches may be used for the surgical management 1. Recurrence is reported to be about 20%-47% [6]. According to Krouse, sinonasal papillomas can be staged as shown in Table 1[7].
){kind=link}
Table 1: Krouse's Staging System for sinonasal papillomas
Kraft's series of 43 sinonasal papillomas were composed of 5 (12%) exophytic, 34 (79%) inverted and 4 (9%) columnar cell types [1]. Since inverted and columnar cell type sinonasal papillomas originate from lateral nasal wall, approaches including medial maxillectomy are suggested for these tumors. As well as endonasal approach, external approach may be preferred for better exposure. Contemporarily, it is stated that endoscopic sinus surgery may be sufficient even for extensive tumors with malignant degeneration. The removal of rhinolith can be done under topical or general anesthesia[8].
In our case, exophytic nasal septal papilloma co-existing with a rhinolith was present. A complete removal of the papilloma and excision of the papilloma was done. In the 9th month follow-up, no recurrence has been determined. Additionally, the presence of a nasal hump may be a clue for traumatic etiology in the development of papilloma as well as for formation of a mechanical barrier facilitating the accumulation of mineral salts to give rise to a rhinolith.
Conclusion
Even though contemporary literature lacks sufficient data, co-existence of rhinoliths and sinonasal papillomas in the same nasal passage made us think that these two separate clinical entities may have triggered the formation of each other. Furthermore investigation and research is necessary to reveal the exact etiopathogenetic relationship between nasal septal papillomas and rhinoliths.Reference
1) Kraft M, Simmen D, Kaufmann T, Holzmann D. Long-term results of endonasal sinus surgery in sinonasal papillomas. Laryngoscope 2003; 113:1541-1547. [ Özet ]
2) Stoney P, Bingham B, Okuda I, Hawke M. Diagnosis of rhinoliths with rigid endoscopy. J Otolaryngol 1991; 20: 6. [ Özet ]
3) Appleton SS, Kimbrough RE, Engstrom HIM. Rhinolithiasis: a review. Oral Surg Oral Med Oral Pathol 1988; 65: 693-698. [ Özet ]
4) Ruprecht A, Wang CM, Rak D. Unsuspected rhinolith. Can Dent Assoc J 1979; 3: 116-117. [ Özet ]
5) O'Dowling IB. A rhinolith perforating the hard palate. J Ir Dent Assoc 1984; 30: 2. [ Özet ]
6) Bielamowicz S, Calcaterra TC, Watson D. Inverting papilloma of the head and neck: the UCLA update. Otolaryngol Head Neck Surg 1993; 109: 71-76. [ Özet ]
7) Krouse JH. Endoscopic treatment of inverted papilloma: safety and efficacy. Am J Otolaryngol 2001; 22: 87-99. [ Özet ]