


CASTLEMAN’S DISEASE OF THE PAROTID: A CASE REPORT
2Ankara Numune Training and Research Hospital, Clinic of Patology, Ankara, Turkey
Summary
Castleman’s disease (CD) is a rare, benign lymphoepithelial diseae of unknown cause, most commonly in the mediastinum. In this article, a 45 year-old male patient with parotid CD is presented and recent update on this entity is discussed. Magnetic resonance imaging scans showed about 3x3 cm mass in the right parotid region. Superficial parotidectomy with en-bloc resection of the mass was performed. Clinically and radiologically no recurrence was noted during a follow up period of one year. Although CD is less frequently seen among the parotid masses, it should be considered in the differential diagnosis of cases with mass in the parotid region.Introduction
Castleman’s disease (CD) is a peculiar type of lymph node hyperplasia and is known by different names including lymphoid hamartoma, giant lymph node hyperplasia, angiofollicular lymph node hyperplasia, angiofollicular hamartoma and benign giant lymphoma [1-3]. Although the mediastinum is their most common location, they also occur in other areas of the body, usually where lymph nodes are normally found [4]. The head and neck is the second most common site for these lesions, but the involvement of the parotid gland is extremely rare [2].In this article, a patient who was found to have CD as a cause of a parotid mass is presented and recent update on this entity is discussed.
Case Presentation
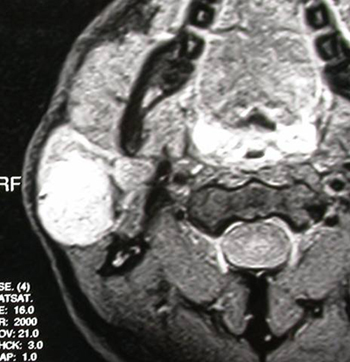
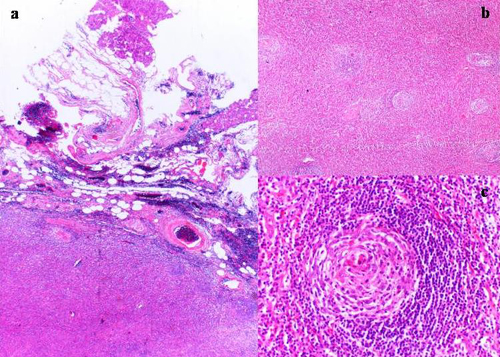
A 45 year-old male patient was referred to our department with a painless swelling in the right parotid region of one year duration. The mass had been rapidly growing for the past two months. Initial physical examination revealed a 4x3 cm mobile, round, firm, non-tender and smooth-surfaced mass with normal overlying skin on the right parotid area. There was no facial weakness, and rest of the head and neck and other systemic examinations were unremarkable.Magnetic resonance imaging scans showed a well-marginated, round, homogenous and highly enhanced 3x3 cm mass in the right parotid gland (Figure 1). Fine-needle aspiration cytology revealed benign lymphoid hyperplasia. Other laboratory examinations were all within normal limits. Superficial parotidectomy with en-bloc resection of the mass was performed and all of the facial nerve branches were preserved. A 5x3x3 cm round mass was located in the superficial parotid gland. The tumor was round and well encapsulated. On sectioning, the cut surface showed a well-encapsulated, grayish brown hard mass. Microscopic examination of the excised mass showed normal parotid tissue with an adjacent mass of a large lymph node (Figure 2a). Normal lymph node architecture was replaced by numerous small follicles, separate cortex and medullary zones were not discernible. There was concentric layering of small lymphocytes around the compact germinal centers, which had hyalinized vessels (Figure 2b). This appearance with dominance of reticulum cells resembled Hassall’s corpuscles. In some part of the germinal centers, “onion-skin” pattern was observed (Figure 2c). The inter-follicular zones contained lymphocytes and plasma cells. And also there was increased inter-follicular vascularity with capillary proliferation and endothelial hyperplasia. A diagnosis of Castleman’s disease of the hyaline vascular type was given.
 Büyütmek İçin Tıklayın |
Figure 1: Axial T2-weighed magnetic resonance imaging scan showing well-marginated, round, homogenous, highly enhanced mass in the right parotid gland. |
 Büyütmek İçin Tıklayın |
Figure 2: Photomicrograph showing the lymphoid proliferation (right) and the parotid gland (left) (a); hyalinized vessels in a germinal centre and concentric layering of small lymphocytes around the germinal center (HE x 200) (b), atrophic germinal centre and onion skinning of the mantle zone lymphocytes (HE x 400) (c). |
Clinically and radiologically no recurrence of disease was noted during a follow up period of one year.
Discussion
Castleman first described the disease in 1956 as a benign solitary lesion under the title of “localized mediastinal lymph node hyperplasia resembling thymoma” [4]. It typically affects young adults between 15 and 35 years of age and has no sex predilection, although it has been reported at any age [1-3].The pathogenesis of this entity is still unknown. Some authors favour a theory of lympho-proliferation due to chronic antigenic stimulation by a virus or chronic inflammation while others consider it to be a lymphoid hamartoma [4]. CD usually presents as a solitary mass, but a complex multicentric variant associated with other systemic features may also be seen [3]. Two histological types are recognized: classic hyaline vascular type (80% to 90% of cases) which is usually unicentric and plasma cell type which can be multicentric and associated with systemic signs, symptoms and other diseases [1-5]. The hyaline vascular type has a benign character and is characterized by prominent proliferation of small blood vessels within the interfollicular areas that often have thick, hyalinized vessels walls and numerous small atrophic follicle centers. The mantle zone of the follicle is well developed and shows a characteristic concentric onion skin layering of lymphocytes. The plasma cellular type is rare, but more aggressive. It is characterized by large follicles with intervening sheets of plasma cells with less vascularity [3,4].
Most lesions (86%) are found in the mediastinum and only %6 is located in the neck [1,4,5]. Within in the head and neck, region, CD most commonly presents as a solitary mass under the sternocleidomastoid muscle or arise as an extension of a mediastinal mass [1,5]. It is also reported in the larynx, tongue, palate, parapharyngeal space, buccal region, and parotid gland [1-5]. In the parotid probably arises in the para-glandular lymph nodes related to the parotid capsule or intra-glandular lymph nodes within the gland parenchyma [1,2]. In the present case the lesion was localized in the superficial lobe indicating that the disease process was taking place in the para-glandular lymph node.
CD of the head and neck, especially parotid, is often a diagnostic challenge. This diagnostic problem can be attributed to a paucity of signs and symptoms and the ability of CD to mimic other neoplasms [1,2,4]. The definitive diagnosis is only possible with histopathologic evaluation [
Surgery is the treatment of choice for the solitary form, whereas chemotherapy, radiotherapy and steroids are proposed for the multicentric type and inoperable cases [1-5]. The use of postoperative radiotherapy (2700-4500 cGy) for potential residual disease has also limited value [5]. No recurrences have been reported in the literature after complete resection of the hyaline vascular type, but a case of recurrence was reported with the plasma cell type in the head and neck [3,4].
Although CD is less frequently seen among the parotid masses, it should be considered in the differential diagnosis of cases with mass in the parotid region.
Reference
1) Goodisson DW, Carr RJ, Stirling RW. Parotid presentation of Castleman's disease: report of a case. J Oral Maxillofac Surg 1997; 55:515-517. [ Özet ]
2) Mohan H, Bal A, Tahlan A. Images in pathology. Castleman's disease of the parotid. J Postgrad Med 2003; 49:348-349. [ Özet ]
3) Somdas MA, Ketenci I, Bicer S, Senturk M, Guney E. Castleman's disease as an unusual neck mass: case report. Ann Otol Rhinol Laryngol 2004; 113:459-461. [ Özet ]
4) Choi G, Lee U, Kim A, Choi JO. Castleman's disease of the parotid gland. J Otolaryngol 1997; 26:319-321. [ Özet ]
5) Sherman JA, Birtwhistle CJ, Davies HT. A rapidly expanding lesion in the neck: unusual presentation of Castleman's disease. Int J Oral Maxillofac Surg 2001; 30:458-460. [ Özet ]