


SOĞUK BIÇAK GLOTTOPLASTİ SES FEMİNİZASYONUNDA BAŞARILI BİR CERRAHİ: OBJEKTİF VE SUBJEKTİF SONUÇLAR
2Uskudar University, Faculty of Health Sciences, Speech and Language Therapy Department, İstanbul, Turkey
3Uskudar University, Faculty of Health Sciences, Odiology Department, İstanbul, Turkey
Özet
Amaç: Soğuk Bıçak Glottoplasti tekniğinin sonuçlarının objektif ve sübjektif olarak değerlendirilmesi.Materyal ve Metod: Çalışmaya 20 erkekten kadına transseksüel dahil edildi. Bütün hastalara feminen bir ses oluşturmak amacı ile endoskopik olarak anterior web oluşturma cerrahisi yani Soğuk Bıçak Glottoplasty uygulandı. Preoperatif ve postoperatif Bazal Frekans (F0) seviyeleri ölçüldü ve karşılaştırıldı. Ayrıca cerrahiden 6 ay sonra hastalara cerrahiden memnuniyetlerini de içeren bir anket uygulandı.
Bulgular: Preoperatif ve postoperatif F0 değerleri ortalaması sıra ile 143,6 ve 237,2 idi. F0 değerlerindeki bu yükselme istatistiksel olarak anlamlı bulundu (p<0.001). Hastaların 14 (%70)'i kişisel değerlendirme anketinde (VAS) 8 puan ve üzerinde değer verdi.
Sonuç: Soğuk Bıçak Glottoplasti, ses feminizasyon cerrahisi seçeneklerinden biridir. Bazal Frekans elevasyonu için güvenilir, etkili ve kolay bir yöntemdir.
Giriş
The voice is one of the communication tools between humans. Basically, the air that coming from the lungs oscillates the vocal folds and forms the primitive sound. Than supralaryngeal vocal tract transforms this sound to voice. These three stations lungs, larynx and supralaryngeal tract varies from person to person and that's why every person have his or her personalized voice. Voice development consists of infancy, childhood, puberty and aging periods. Newman et al [1] showed that the laryngeal mucosa and deeper tissues have estrogen, progesterone, and androgen receptors. This means that sexual hormones influences the vocal characteristics. During puberty male larynx enlarges and drops to a lower level in the neck. These new position of the larynx causes Fundamental Frequency (F0) levels drop around 100 Hz [2]. Markova et al [3] observed morphology of voice-related structures during puberty with MRI and reported that puberty has a strong effect in both vocal fold and vocal-tract length in males; which has not seen in females.Transsexualism is a gender identity disorder in which patients feel that they are trapped in the body of the wrong sex [4]. They usually seek medical interventions to change their body to the opposite gender. Landen [4] reported that the prevalence of this situation is 3/1 male to female in 1990s. In 21th century the transsexuals gain more acceptable position in the big population and so nowadays we see more male-to-female transsexual (MFT)s got surgeries. The transformation surgery is a complex procedure that contains psychiatric, plastic and reconstructive and hormonal therapies. After gender transformation the masculine voice of MFTs makes a handicap to be accepted as female. At that time they start to search an Otolaryngologist to solve this problem.
There were two ways for Pitch raising. One is voice therapy without surgery, and the second one is surgery. Voice therapy can help to increase the pitch in controlled situations but in uncontrolled situations like yawning, laughing, coughing and sneezing male voice reappears [5]. Surgery is more efficient in uncontrolled situations. The theory in surgery relies on elongating the vocal folds to increase the tension or decreasing the vibrating portion of the vocal folds. The Cricothyroid Approximation (CTA) is the procedure that increases the tension over vocal folds by fixing cricoid cartilage to thyroid cartilage. The vocal folds' vibrating portion can be decreased by forming a web at the anterior 1/3 portion of the vocal folds. This web could be formed by cold-knife or by laser reduction as described by Wendler [5,6,7,8.9]. In this paper we have performed cold knife glottoplasty to MFTs and demonstrated advantages, disadvantages, and patient satisfaction of the procedure.
Yöntem ve Gereçler
Study was approved by the instutional ethics committee (Number 87/2017). Informed consent was obtained from all participants included in the study.This is prospective study of patients treated for male voice change in both hospitals between January 2016 to September 2017. 20 MFT are accepted in the study. Before surgery all patients had psychiatric evaluation. None of the patients had preoperative speech therapy. All patients were treated with cold-knife glottoplasty technique [5]. Pitch levels of all patients were obtained before surgery and at the 6th month after surgery. At the 6th month of follow up all patients were undergone a survey of self-satisfaction for the results. The survey consisted of 4 questions. First one was Visual Analogue Scale from 1-10 for personal satisfaction from the operation. Second was about the surroundings finding about the new voice as female. Third one was about the recognition as female during telephone calls. The last one was about the recovery time from the surgery. The answers for last three questions were "yes" or "no".
Vocal Assessment
All patients were evaluated at the speech lab of Ministry of Health University Gaziosmanpasa Taksim Education and Research Hospital. The vocal assessment process consists of
1. Laryngostroboscopic evaluation (Xion Endo-Stroboscope, Endostrop DX. Munich, Germany) of the vocal folds.
2. Pitch (Fundamental Frequency, F0) measurement: The patients were asked to pronounce /a/ sound at comfortable pitch and loudness for 5 sec. The sound was recorded by a microphone (Audio-Technica AT2005USB Cardioid Dynamic USB/XLR Microphone, Audio-Technica U.S., Inc.) which was placed 5 cm from the mouth. Digitally recorded data were transferred to a PC at a sampling rate of 44.1 kHz. Measurements were done with Praat (Boersma, P& Weenink, D, 2013, Version 5.2.21, www.praat.org) application.
Surgical Procedure
The operations were performed by the same senior surgeon (KY). All of the operations were done under general anesthesia with endotracheal intubation. After suspension laryngoscopy anterior commissure was visualised and procedure was carried out under microscopic guidance. One of the most important parts of the surgery is complete visualization of the vocal folds. To achieve this external manipulation of the larynx can be performed. The vocal folds were visualised completely and palpated for misdiagnosed submucosal lesions. The anterior 1/3 of the vocal folds were determined. Posterior end of the anterior 1/3 was grasped by Bouchayer forceps and moved medially. The epithelium was stripped anteriorly through the anterior commissure by microscissors. The stripped epithelium was removed and same procedure was carried out to the opposite site of the vocal fold. After hemostasis, deepithelialised vocal folds were sutured to each other with 6/0 vicryl sutures starting from anterior commisssure. Usually three or four sutures were suitable for anterior glottic web formation. Tissue adhesives were not used. After surgery patients were advised for complete voice rest for seven days. No extra medications were given to patients. None of the patients had dspnea after surgery.
Patients were controlled 1 week, 1 month and 6 month after surgery at the speech lab. None of the patients wanted to have speech therapy courses.
Statistical Analysis
Normalisation control is undergone by drawing graphics with Shapiro Wilk test, histogram, Q-Q plot and box plot. The data are given as standard deviation, minimum, maximum, frequency and percentage. The differences between the preoperative and postoperative pitch levels are evaluated by Wilcoxon test. Significance interval is taken with p<0.05 and bidirectionally. NCSS 10 (2015. Kaysville, Utah, USA) program is used for analysis.
Bulgular
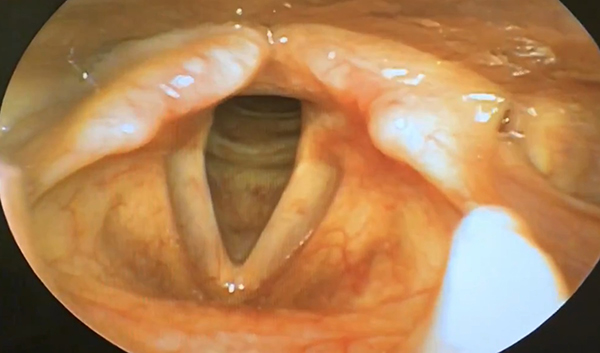
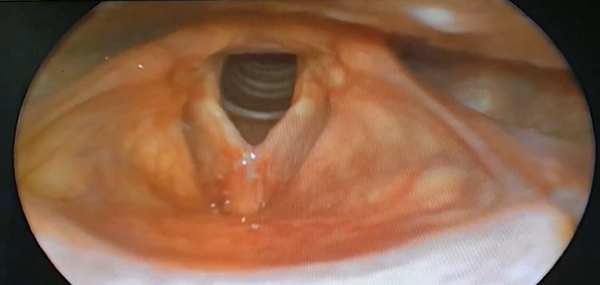
20 MFTs included in the study. The mean age of patients was 25,70 (20-39). 9 (45%) of them were smokers. All patients were controlled 1 week after surgery. At the laryngostroboscopic evaluation the formation of the anterior web was observed (Picture 1 and 2). Neither of the patients needed a second surgery. There were no early and late complications like suture fading, breathiness problems or granuloma formation till the 6 months after operation. 14 (70%) of the patients gave 8 points or more in self-satisfaction VAS score, meaning that they were satisfied from the result. 18 (90%) of the patients reported that their surroundings were noticed the change in their voice. Also 18 (90%) patient reported that they were recognised as female during phone calls. 9 (45%) of the patients returned to work 1 week later, 7 (35%) in 1-3 weeks and others in more than 3 weeks (Table 1). The mean preoperative and postoperative pitch levels were 143,6 Hz and 237,2 respectively. The change in pitch levels were statistically significant (p<0.001) (Table 2).){kind=link}
){kind=link}
 Büyütmek İçin Tıklayın |
Picture 1: Preoperative laryngoscopic view |
 Büyütmek İçin Tıklayın |
Picture 2: Postoperative Laryngoscopic view at 6th month after surgery |
Table 1: Patients data before and after surgery.
Table 2: Statistics of preoperative and postoperative pitch.
Tartışma
The human voice is one of the instruments for communication. A careful listener can obtain some characteristics of the person such as age, sex and physical state by only listening. The larynx is almost identical for both sexes in childhood. But during puberty larynx enlarges and vocal tract elongates [10]. By the end of maturation, vocal fold length becomes approximately 1,6 cm in adult males and 1.0 cm in adult females [11]. As the length of the vocal folds increase, its vibration rate decreases resulting in lower Fundamental Frequency (F0) and vice versa [10,11]. The masculinity of the voices of MFTs is one of the problems after gender reassignment surgery. The lack of harmony between their physical appearance and voices reduces their social acceptance. That's why many MFTs seek help from Otolaryngologist or voice surgeon after gender reassignment surgery.Androgen therapy can change the voice of Female-to-Male transgenders, but estrogen has no such effect in MFTs [7]. Due to the ineffectiveness of hormonal therapy, surgery and/or speech therapy stands as the only weapon for voice change. Speech therapy is noninvasive and helps patients to adopt changes in their life. But most MFTs do not satisfied from therapy alone [12]. The goal of the surgery is to elevate the pitch of the patient. Spencer [13] described that average pitch elevation must be about 100-150 Hz to be perceived as female for MFTs. Cricothyroid approximation, Anterior glottal web formation and laser reduction glottoplasty were the most popular techniques for this purpose. They can be used in combination with or without speech therapy [5,6,7,8,12,14,15]. As authors we tried Cold-Knife Glottoplasty as we thought it is easy to perform, has less morbidity and more successful than other surgeries alone.
In this research we used a survey for subjective analysis. The survey contains 4 questions. First one was a VAS scale from 1-10 for overall satisfaction of their new voice. 14 of the patients scored 8 or more points that meant they satisfied from the result. This result resembles the result of Yılmaz et al. [15]. In their research 20 of 27 patients (74%) characterized their voice as female. Second question was, as if their relatives found their voice as female. 18 (90%) of them reported a positive result which was a good response for social acceptance. This question was used in survey because we think that the positive response from their relatives or friends could give a better satisfaction from the resultant voice. The third question have asked whether any change in telephone conversations. 18 (90%) of the patients reported that in telephone conversations they were thought as female. Yılmaz et al [15] recorded the voices of the patients and medical students listened these voices. They reported 85% of the voices were as female. These rates are similar to our research.
The theory of cold-knife glottoplasty relies on shortening of both the vibrating surface of the vocal folds and laryngeal diameter. The shortening of the vibrating surface of the vocal folds leads an increase in the fundamental frequency (F0). This decrease in laryngeal surface does not have a negative affect on breathing at rest or at exercise [8]. The voice is accepted as female as the fundamental frequency is above 160 Hz [13]. In our research the mean F0 of the patients increased significantly (average 94 Hz). This gain in average F0 is similar to other researches in literature that used Wendler Glottoplasty, Mastronikolis et al [8], Casado et al [9], Anderson et al [10], Yılmaz et al [15].
All of the patients stayed one night at the hospital after surgery. None of them got any early complication after surgery. Most of the patients recovered early from the surgery and 9 (45%) of them returned to work in one week. There was not any major complication like suture problems or need for second surgery. After surgery the patients refused to take speech therapy. We have failed in two patients. These two patients final F0 was 158,509 Hz and 154,785 Hz. These patients had anatomically good results and an anterior web is formed, but there were a lack of functionality and they did not have a female voice. Speech therapy or a different type of surgical procedures may be applied to them.
We did not used Voice Handicap Index (VHI) for self satisfaction in this research. Because they did not have any voice diseases and they did not suffer from dysphonia, breathiness or failure in conversations. This is one of the differences of our research. Because there is a conflict in literature for the use of VHI for these people. According to Mastronikolis [8] and Remacle [12]'s work there was not any difference in VHI scores. They declared that VHI is not sensitive enough for these patients, But Yılmaz [15] recorded a significant change in VHI. Some researchers reported a new questionnaire as Transgender Self-evaluation Questionnaire (TSQ) [16]. But we do not have a validated Turkish version of that questionnaire so we could not use it for subjective evaluation.
Sonuç
Nowadays, there is an increase in social acceptance of transgendered persons. Most of them are MTFs. Cold-knife Glottoplasty is one of the surgical options for voice feminization. It is safe and effective method for pitch elevation. There is not any scar formed after the surgery. This paper contains results of 20 MFTs who had undergone cold-knife glottoplasty operation. At the 6th month follow up we had good results as approximately 100 Hz mean pitch elevation. We think that every voice surgeon should have the ability to do this operation for voice feminisation.Ethical approval: Study was approved by the ethics committee of Ministry of Health University Gaziosmanpasa Taksim Education and Research Hospital (Number 87/2017).
Informed consent was obtained from all participants included in the study.
Kaynaklar
1) Newman SR, Bulter J, Hammond EH, Gray SD. Preliminary report on hormone receptors in the human vocal fold. J Voice. 2000;14(1):72-81.
2) Franca MC, Bass-Ringdahl S. A clinical demonstration of the application of audiovisual biofeedback in the treatment of puberphonia. Int J Pediatr Otorhinolaryngol. 2015 Jun;79(6):912-20. doi: 10.1016/j.ijporl.2015.04.013. Epub 2015 Apr 16. [ Özet ]
3) Markova D, Richer L, Pangelinan M, Schwartz DH, Leonard G, Perron M, Pike GB, Veillette S, Chakravarty MM, Pausova Z, Paus T. Age- and sex-related variations in vocal-tract morphology and voice acoustics during adolescence. Horm Behav. 2016 May;81:84-96. doi: 10.1016/j.yhbeh.2016.03.001. Epub 2016 Apr 8
4) Landén M, Wålinder J, Lundström B. Prevalence, incidence and sex ratio of transsexualism.Acta Psychiatr Scand. 1996 Apr;93(4):221-3.
5) Gross M. Pitch-raising surgery in male-to-female transsexuals. J Voice. 1999 Jun;13(2):246-50
6) Wendler J. Vocal pitch elevation after transexualism male to female. In: Proceedings of the Union of the European Phoniatricians; Salsomaggiore, Italy, 1990.
7) Van Damme S, Cosyns M, Deman S, Van den Eede Z, Van Borsel J. The Effectiveness of Pitch-raising Surgery in Male-to-Female Transsexuals: A Systematic Review. J Voice. 2017 Mar;31(2):244.e1-244.e5. doi: 10.1016/j.jvoice.2016.04.002. Epub 2016 Jul 28.
8) Mastronikolis NS, Remacle M, Biagini M, Kiagiadaki D, Lawson G. Wendler glottoplasty: an effective pitch raising surgery in male-to-female transsexuals. J Voice. 2013 Jul;27(4):516-22. doi: 10.1016/j.jvoice.2013.04.004.
9) Casado JC, O'Connor C, Angulo MS, Adrián JA. Wendler glottoplasty and voice-therapy in male-to-female transsexuals: results in pre and post-surgery assessment. Acta Otorrinolaringol Esp. 2016 Mar-Apr;67(2):83-92. doi: 10.1016/j.otorri.2015.02.003.
10) Markova D, Richer L, Pangelinan M, Schwartz DH, Leonard G, Perron M, Pike GB, Veillette S, Chakravarty MM, Pausova Z, Paus T. Age- and sex-related variations in vocal-tract morphology and voice acoustics during adolescence. Horm Behav. 2016 May;81:84-96. doi: 10.1016/j.yhbeh.2016.03.001. Epub 2016 Apr 8.
11) Titze IR. Physiologic and acoustic differences between male and female voices. J Acoust Soc Am. 1989 Apr;85(4):1699-707.
12) Remacle M, Matar N, Morsomme D, Veduyckt I, Lawson G. Glottoplasty for male-to-female transsexualism: voice results. J Voice. 2011 Jan;25(1):120-3. doi: 10.1016/j.jvoice.2009.07.004. Epub 2010 Feb 19. [ Özet ]
13) Spencer LE. Speech characteristics of male-to-female transsexuals: a perceptual and acoustic study. Folia Phoniatr (Basel). 1988;40(1):31-42. [ Özet ]
14) Song TE, Jiang N. Transgender Phonosurgery: A Systematic Review and Meta-analysis. Otolaryngol Head Neck Surg. 2017 May;156(5):803-808. doi: 10.1177/0194599817697050. Epub 2017 Mar 28. [ Özet ]
15) Yılmaz T, Kuşçu O, Sözen T, Süslü AE. Anterior Glottic Web Formation for Voice Feminization: Experience of 27 Patients. J Voice. 2017 Mar 31. pii: S0892-1997(17)30061-9. doi: 10.1016/j.jvoice.2017.03.006. [ Özet ]