


SINUS TYMPANI VOLUME IN TEMPORAL BONES WITH KÖRNER'S SEPTUM: A QUANTITATIVE THREE- DIMENSIONAL ANALYSIS
2Ondokuz Mayis University Faculty of Medicine, Department of Radiology, Samsun, Turkey
3Giresun University, Faculty of Medicine, Department of Radiology, Giresun, Turkey
4 Giresun University, Faculty of Medicine, Department of ENT, Giresun, Turkey
Summary
Purpose: The aim of this retrospective- archival temporal bone computerized tomography study was to investigate the effects of Körner's septum on sinus tympani development.Methods: We included 68 temporal bones with Körner's septum from 38 patients and 72 temporal bones without Körner's septum from 38 other patients. Using OsiriX software for MacOS (version 3.8.1, Pixmeo), we measured the volumes from three- dimensional sinus tympani models and compared the sinus tympani volumes between the temporal bones with and without Körner's septum.
Results: Among 427 patients totally reviewed, 38 (8.9 %) had Körner's septum. The median sinus tympani volume was 8.3 (1.7- 20.3) mm3 in temporal bones with Körner's septum and 14.2 (2.1- 53.2) mm3 in temporal bones without. The sinus tympani volume was significantly lower in temporal bones with Körner's septum compared to those without (p<0.001). We found that Körner's septum had negative effects on sinus tympani development since was associated with smaller sinus tympani.
Conclusion: Patients with Körner's septum had a lower sinus tympani volume associated with the decreased risk of residual cholesteatoma. Beside the removal of primary disease, effective drilling of Körner's septum during cholesteatoma surgery would be sufficient to provide the pneumatization of mastoid antrum and middle ear, resulting in decreased risk of residual disease.
Introduction
The petrosquamous lamina, also known as Körner's septum, is a dense bone plate dividing the mastoid process into superficial squamous and deeper petrosal portions [1]. The first description of the Körner's septum belongs to Cheattle [2], however, the clinical significance of this structure was reported by Körner in 1926 [3]. During the developmental process of the antrum and mastoid cavity, Körner's septum usually begins to resolve and completely disappear [4]. The persistence of the Körner's septum might represent a developmental failure of the temporal bone [5]. Several studies focused on the clinical significance, anatomy and variations of the Körner septum in the prior literature [2,4,6]. In addition, the association between Körner's septum and mastoid aeration was reported [7]. In this context, Körner's septum might be considered as a developmental failure associated with the development of the spaces with a high surgical implication, like the sinus tympani. Given that the sinus tympani is known to be related to the risk of residual cholesteatoma due to the difficulty of visualization by conventional light microscopy, an association between the persistence of Körner's septum and the size and shape of the sinus tympani might have a clinical and/or surgical implication.The aim of this retrospective- archival temporal bone study was to investigate the effects of the persistence of Körner's septum on sinus tympani development, analyzing the sinus tympani volume of the temporal bones with Körner's septum upon 3- dimensional (3D) reconstruction models, in comparison with the temporal bones without.
Methods
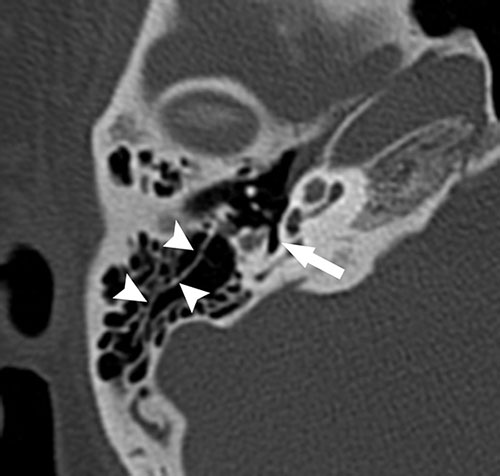
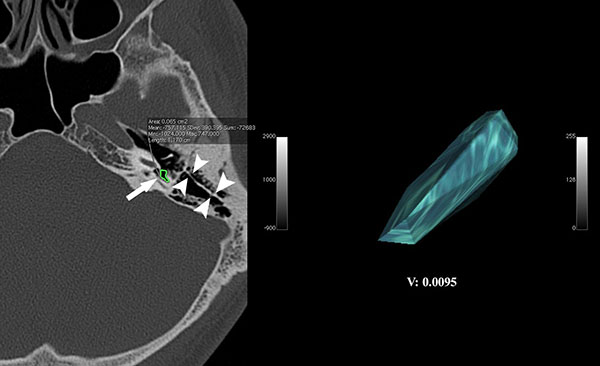
Study Design and 3D volumetric analysisThis retrospective- archival, temporal bone computed tomography (CT) study was approved by the local ethical committee and conducted in line with the dictates of the World Medical Association Declaration of Helsinki. We searched the temporal bone CT studies of 427 patients between January 2018- May 2019 from the radiological archive of our institution to identify cases with Körner's septum (Fig I). Excluded from the study were the patients with the following conditions that might cause difficulty in measurement and 3D volumetric analysis of sinus tympani: history of temporal bone trauma, otologic surgery, cholesteatoma, and chronic otitis media. We obtained the data using a 16-slice CT unit (Somatom Emotion; Siemens, Munich, Germany) with Picture Archiving Communication Systems (PACS) (Akgun, Ankara, Turkey). The parameters of the CT scanner were 130 kVp, 1.2 mm slice thickness, 0.8-s rotation time, and 1 mm pitch. A five-year experienced radiologist measured the sinus tympani volumes quantitatively using the OsiriX software for MacOS (version 3.8.1, Pixmeo) and its volumetric function. This was based on manual segmentation of sinus tympani by tracing the borders of it in each of the contiguous CT slices using an Osirix pencil tool. At the end of segmentation process, the volume was calculated using the calculate volume function of the software and a 3D diagram was created. We created a 3D volume diagram of the sinus tympani (Fig II) and presented the volume in mm3. Firstly, we constituted two groups according to the presence of Körner's septum: Körner's septum group (consisted of the temporal bones with Körner's septum) and the control group (consisted of the temporal bones without Körner's septum). Then, we compared the sinus tympani volumes of the groups.
 Büyütmek İçin Tıklayın |
Figure I: Körner's septum (arrow heads) and sinus tympani (arrow) in axial CT section |
Statistical Analysis
Results are presented as median (min- max). The abnormal distribution of data was confirmed using Kolmogorov- Smirnov normality test (p<0.001). To compare the sinus tympani volumes between the Körner's septum group and the control group, we used Mann Whitney- U test. We used SPSS software for Windows (SPSS Inc, Chicago, IL) for statistical analysis. We considered a P value less than 0.05 statistically significant.
Results
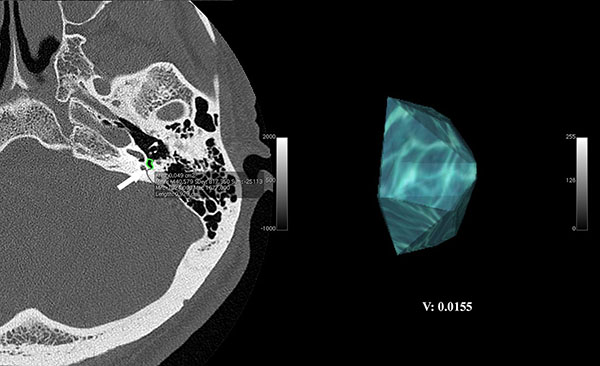
We totally reviewed 427 patients, and 38 had Körner's septum. The prevalence of Körner's septum was 8.9%. Thirty- eight patients with Körner's septum (21 males and 17 females, mean age: 40 ± 16 years years) as study group and 38 other patients without Körner's septum (20 males and 18 females, mean age: 37 ±17 years) as control group were eligible for the study. Of 38 patients with Körner's septum, 8 (21 %) had unilateral and 30 (79 %) had bilateral Körner's septum. The groups were age and gender matched (p = 0.34 and p = 0.81, respectively). The study group consisted of 68 temporal bones with Körner's septum from 38 patients and the control group consisted of 72 temporal bones without Körner's septum from 38 other patients (control group). Only 6 (8.8%) out of 68 (91.2%) temporal bones had an incomplete Körner's septum. The median sinus tympani volume was 8.3 (1.7- 20.3) mm3 in temporal bones with Körner's septum (Fig II) and 14.2 (2.1- 53.2) mm3 in temporal bones without Körner's septum (Fig III). The sinus tympani volume was significantly lower in temporal bones with Körner's septum compared to those without (p<0.001). Thus, we found that Körner's septum had negative effects on the sinus tympani development since was associated with smaller sinus tympani.
 Büyütmek İçin Tıklayın |
Figure II: 3D reconstruction diagram of the sinus tympani (arrow heads) in a temporal bone with Körner's septum (arrow). (Sinus tympani volume: 9.5 mm3) |
 Büyütmek İçin Tıklayın |
Figure III: 3D reconstruction diagram of the sinus tympani (arrow heads) in a temporal bone without Körner's septum. (Sinus tympani volume: 15.5 mm3) |
Discussion
In this modern era of otologic surgery, developmental associations between the landmarks, spaces and various structures of the temporal bone might have surgical implications that lead surgeons to perform more effective and curative cholesteatoma surgery without any intraoperative complication. Both persistence of the Körner's septum and sinus tympani size might determine the surgical approach to the cholesteatoma. Based on the hypothesis that the persistence of the Körner's septum might negatively affect the development of the sinus tympani and the relevant structures as a developmental disorder, we investigated the sinus tympani volumes in temporal bones with Körner's septum compared to the temporal bones without. The volume of sinus tympani was significantly lower in temporal bones with Körner's septum. Lower sinus tympani volume in temporal bones with Körner's septum might be associated with the decreased risk of residual cholesteatoma, however, beside the removal of primary disease, effective drilling of Körner's septum and the other structures that might be an obstacle for pneumatization remains important to provide an adequate pneumatization of the middle ear and mastoid cavity. Although residual disease originating from the sinus tympani might not be the main problem of cholesteatoma surgery in temporal bones with Körner's septum, removal of the disease from the sinus tympani should not be omitted.Surgeons usually encounter Körner's septum during antrostomy because it is not rare. According to the report by Goksu et al., overall prevalence of Körner's septum was 20.53% [4]. In our study, the prevalence of Körner's septum was lower as 8.9%. Körner's septum represents the persistence of the petrosquamous suture line and it might be associated with the Cog process, which is the middle bone portion of the petrosquamous lamina occasionally seen in tegmen tympani [8]. Previous studies focusing on the Cog and related structures suggested that Cog process had a potential for attic blockage increasing the risk of attic retraction pockets and cholesteatoma [9,10]. Thus, the presence of the Körner's septum might also increase the risk of cholesteatoma. Additionally, Körner's septum may create obstacles during mastoid surgery, a false antrum can be found, and facial nerve can be injured. Finding a false antrum during mastoidectomy can prevent the complete removal of the disease. Remnant of a Körner's septum can inhibit adequate pneumatization of the middle ear, resulting in residual disease. Therefore, Körner's septum is a structure mainly associated with residual cholesteatoma. Because of the decreased volume of sinus tympani in temporal bones with Körner's septum, the risk of residual disease might not depend on the sinus tympani, even the sinus tympani is known to be the most common site of residual cholesteatoma. According to Ozturan et al, retrofacial approach to the sinus tympani would be more accurate to eradicate hidden cholesteatoma [11]. Thomassin et al. stated that blind dissection of sinus tympany via light microscopy may result in residual cholesteatoma or injury of high jugular bulb or dehiscent facial canal [12]. In the temporal bones with Körner's septum, this risk naturally decreases due to shallower sinus tympani, but surgeons should keep the increased complication and residual cholesteatoma risk in mind due to the basic anatomical characteristics of Körner's septum. Nevertheless, endoscopic examination of sinus tympani absolutely decreases the risk of residual cholesteatoma because it provides an opportunity of direct evaluation. Additionally, transcanal endoscopic access allows better understanding of anatomy, function and spreading characteristics of the disease.
In previous radio- anatomical studies, associations of sinus tympani and Körner's septum with mastoid pneumatization were reported using 2- dimensional (2D) CT sections. The 2D study by Baklaci et al. [13] revealed the association between deeper sinus tympani and well- pneumatized mastoid bone. Toros et al. [7] used 2D CT sections to investigate the association between mastoid aeration and Körner's septum. Two- D CT sections were also used by Ozcan et al.[14,15] and Kayabasi et al. [16], to investigate the variations of developmental disorders of paranasal sinuses. However, unlike previous publications, we used a novel technique that might more accurately determine the size, shape and volume of air- filled spaces like the sinus tympani. The quantitative 3D analysis method used in this study would be a new horizon for anatomists as well as surgeons, in further radio- anatomical studies. Additionally, 3D analysis method is suitable for reconstruction studies using histopathologic temporal bone sections [17,18]. However, this study was not capable of figuring the causative mechanism of the association out, and this might be considered the only limitation of our study.
Conclusion
In conclusion, patients with Körner's septum had a lower sinus tympani volume associated with the decreased risk of residual cholesteatoma. Beside the removal of primary disease, effective drilling of Körner's septum during cholesteatoma surgery would be sufficient to provide the pneumatization of mastoid antrum and middle ear, resulting in decreased risk of residual disease.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
FINANCIAL DISCLOSURE
The authors declared that this study has received no financial support.
Reference
1) Shulman A, Rock EH. Korner's (petrosquamous) septum in otology. Report of five cases. Arch Otolaryngol 1972; 96: 124-129. [ Özet ]
2) Cheattle A. The surgical anatomy of the temporal bone. London: J&A Churchill Ltd, 1907.
3) Korner O. Das septum petrosquamousum(mastoideum) und seine klinische bedeutung Arch Ohren Nasen Kehlkopfheilk 1926; 17: 137.
4) Göksu N, Kemaloglu Y, Köybasioglu A, Ileri F, Özbilen S, Akyildiz N. Clinical importance of the Korner's septum. American Journal of Otology -New York 1997; 18: 304-306.
5) Proctor B, Nielsen E, Proctor C. Petrosquamosal suture and lamina. Otolaryngol Head Neck Surg 1981; 89: 482-495. [ Özet ]
6) Wojciechowski T, Skadorwa T, Drozdz A, Ciszek B, Szopinski K. The radioanatomical assessment of the Korner's septum. Surg Radiol Anat 2019; 41: 669-673. [ Özet ]
7) Toros SZ, Karaca CT, Habesoglu TE, Noseri H, Ertugay CK, Naiboglu B, Egeli E. Is there a relation between mastoid aeration and Korner's septum? Eur Arch Otorhinolaryngol 2010; 267: 1523-1526. [ Özet ]
8) Ozer E, Bayazit YA, Kara C, Mumbuc S, Kanlikama M, Gumusburun E. Korner's septum (petrosquamosal lamina) and chronic ear disease. Surg Radiol Anat 2004; 26: 118-121. [ Özet ]
9) Hoshino T. Surgical anatomy of the anterior epitympanic space. Arch Otolaryngol Head Neck Surg 1988; 114: 1143-1145. [ Özet ]
10) Hoshino T, Suzuki JI. Anterior attic wall anatomy. Arch Otolaryngol 1978; 104: 588-590. [ Özet ]
11) Ozturan O, Bauer CA, Miller CC, 3rd, Jenkins HA. Dimensions of the sinus tympani and its surgical access via a retrofacial approach. Ann Otol Rhinol Laryngol 1996; 105: 776-783. [ Özet ]
12) Thomassin JM, Korchia D, Doris JM. Endoscopic-guided otosurgery in the prevention of residual cholesteatomas. Laryngoscope 1993; 103: 939-943. 13) Baklaci D, Kuzucu I, Guler I, Akbal S, Kum NY, Yildirim GK, Parlak IS, Kum RO, Ozcan M. Effect of mastoid bone pneumatization on the conformation and depth of the sinus tympani, a high-resolution computed tomography study. Surg Radiol Anat 2019. [ Özet ]
14) Ozcan KM, Hizli O, Sarisoy ZA, Ulusoy H, Yildirim G. Coexistence of frontal sinus hypoplasia with maxillary sinus hypoplasia: a radiological study. Eur Arch Otorhinolaryngol 2018; 275: 931-935. [ Özet ]
15) Ozcan KM, Hizli O, Ulusoy H, Coskun ZU, Yildirim G. Localization of orbit in patients with maxillary sinus hypoplasia: a radiological study. Surg Radiol Anat 2018; 40: 1099-1104. [ Özet ]
16) Kayabasi S, Hizli O, Ozkan D. Does paranasal sinus development affect olfactory fossa depth and lateral lamella length? Laryngoscope 2019. [ Özet ]
17) Monsanto RD, Pauna HF, Kaya S, Hizli O, Kwon G, Paparella MM, Cureoglu S. Epitympanum volume and tympanic isthmus area in temporal bones with retraction pockets. Laryngoscope 2016; 126: E369-e374. [ Özet ]