


INVESTIGATION OF THE FUNCTIONALITY OF FUKUDA STEPPING TEST IN DIZZINESS PATIENTS
2Karabuk University Training and Research Hospital, Department of Audiology, Karabuk, Turkey
Summary
Objective: The aim of this study was to determine the sensitivity and specificity of Fukuda stepping test (FST), which is used to evaluate vestibular asymmetry in patients with dizziness.Materials and Methods: The vestibular evaluation forms of 189 patients admitted to the otorhinolaryngology outpatient clinic with dizziness between October 2017 and October 2019 were retrospectively reviewed. FST results were compared with caloric test results, which is accepted as the gold standard method to evaluate vestibular dysfunction. The specificity, sensitivity, positive predictive value and negative predictive value of FST were calculated.
Results: Of the 189 patients, 117 were female (61.9%) and 72 were male (38.1%). The mean age was 41.06 ± 13.42 years (range, 15-72 years). There was a significant relationship between caloric test results and FST (p <0.001). The sensitivity and specificity of FST were 53.3% and 78.6%, respectively. The positive predictive value for FST was 32.0% and the negative predictive value was 89.9%.
Conclusion: FST alone is not a reliable screening test to detect unilateral vestibular dysfunction. In addition to FST, other bedside vestibular tests should be performed to obtain sufficient information about vestibular pathology in patients with dizziness.
Introduction
The vestibular system senses physical activities in daily life and regulates eye, neck and body movements in accordance with these activities. The vestibulo-ocular reflex provides the fixation of the eye by controlling the agonist-antagonist extraocular muscles during head movements[1]. The vestibulo-colic reflex is formed by transmitting inputs from otolithic organs and semicircular canals to the neck muscles and stabilizing the head. The vestibulo-spinal reflex (VSR) controls the extensor and flexor skeletal muscles via lateral and medial vestibulospinal tracts and provides body stabilization in dynamic movements[2]. In vestibular system diseases, pathology is observed in these reflexes. Therefore, examination of these reflexes is of great importance to determine whether the pathology is peripheral or central in patients presenting with dizziness or vertigo.The Fukuda stepping test (FST), also known as the Unterberger test, is a test used to evaluate VSR gain asymmetry due to labyrinth dysfunction. FST can be applied quickly and easily in patients presenting with dizziness complaints to outpatient clinics. The caloric test is considered the gold standard method for identifying peripheral vestibular dysfunction[3]. However, the caloric test is time-consuming and uncomfortable for patients. In addition, caloric test cannot be performed in patients with canal wall down tympanomastoidectomy, severe eye movement defects and eye prosthesis. Therefore, FST is still frequently used as a screening test in neurology and otorhinolaryngology outpatient clinics to evaluate peripheral vestibular dysfunction. However, sometimes caloric test and FST results are incompatible with each other. Therefore, the reliability of FST is controversial.
In this study, we aimed to determine the functionality of FST by comparing FST and caloric test results in patients presenting to the otorhinolaryngology outpatient clinic with dizziness.
Methods
Patients selectionIn this study, patients who presented to the otorhinolaryngology outpatient clinic with dizziness between October 2017 and October 2019 were evaluated retrospectively. The vestibular evaluation forms of the patients were scanned from the archive. Patients who underwent caloric test, FST and Romberg test were included in the study. Patients who did not have any of these tests and patients with pathological Romberg test were excluded from the study. In addition, patients with orthopedic disorders, patients with central vestibular pathology, and patients with a previous history of otologic surgery were excluded. 189 patients who met all criteria were included in the study. Caloric test results and FST results were compared. Sensitivity, specificity, positive and negative predictive values of FST were calculated. Ethical approval for the study was obtained from the ethics committee of our institution (2019/5). The study was performed in accordance with principles of Helsinki Declaration.
Romberg test
The Romberg test was performed on a hard floor for all patients. The patients were asked to stand upright, hang their arms to their sides and join their feet together. Patients were asked to keep their balance in this position for 30 seconds with their eyes closed. A stopwatch was used to record the duration of the patient's stability during the test. The test was considered abnormal in patients who opened their eyes within thirty seconds, stepped to avoid falling, and could not stabilize.
Fukuda stepping test (FST)
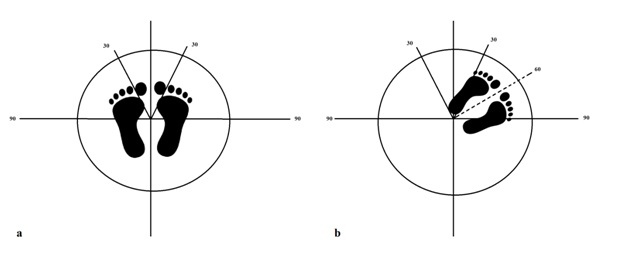
For FST, patients were asked to take off their shoes, stand upright, extend their arms forward, and take 50 steps on the same spot with their eyes closed. At the end of 50 steps, the degree of rotation was measured according to the initial position. Rotation to one side (right or left) of more than 30 degrees was considered abnormal (dysfunction of the vestibular organ on the rotation side) (Figure 1).
 Büyütmek İçin Tıklayın |
Figure 1: Fukuda stepping test, a. starting position, b. final position after 50 steps |
Caloric test
Caloric test was performed with Aquastar air caloric device. The test was performed in the supine position and the head of the patient was flexed 30 degrees. The test was carried out by giving bitermal cold (27 ° C) and warm (47 ° C) air. Cold and warm air was applied to each external ear canal for 60 seconds and nystagmus was recorded with a Micromedical brand videonistagmography (VNG) device (Spectrum 5, Chatham, USA). The caps of the VNG goggles were closed and the patient was asked to count to 50 to prevent fixation during the test. The artifacts formed during the recording were removed and the maximum slow phase velocities of the nystagmus formed during each irrigation were selected. Jongkees' formula was used to diagnose canal paresis[4]. A slow phase rate of more than 25% nystagmus between two ears was considered as the criterion for the diagnosis of unilateral vestibular dysfunction (UVD) in the caloric test.
Statistical analysis
SPSS 21.0 (SPSS software, Chicago, USA) was used for statistical analysis. Descriptive statistics were given as mean, standard deviation, median, minimum, maximum and percentage values. Chi-square test was used to evaluate the relationship between caloric test and FST. P <0.05 was considered statistically significant.
Results
Of the 189 patients included in the study, 117 (61.9%) were female and 72 (38.1%) were male. The mean age was 41.06 ± 13.42 years (range, 15-72 years). According to the caloric test result, UVD was present in 30 patients (15.9%), 17 of them (9.0%) on the right side and 13 (6.9%) on the left side. The caloric test results of 159 patients (84.1%) were normal. FST was lateralized on the right side in 24 patients (12.7%) and on the left side in 30 patients (15.9%). 135 patients (71.4%) had normal FST.There was a significant relationship between caloric test results and FST (p <0.001). In 16 (53.3%) of 30 patients with UVD detected by caloric test, FST pathology was seen in the same direction. In 4 patients (13.30%), FST showed rotational movement in the opposite direction with caloric test result. In 10 patients (33.3%), although the caloric test was abnormal, the FST was normal. FST was normal in 125 (78.6%) of 159 patients with normal caloric test results. However, FST was abnormal in 34 patients (21.4%), although caloric tests were normal. The caloric test and FST results of the patients are given in Table 1. The sensitivity and specificity of FST were 53.3% and 78.6%, respectively. The positive predictive value for FST was 32.0% and the negative predictive value was 89.9%.
){kind=link}
Table 1: Caloric test and Fukuda stepping test (FST) results
Discussion
In this study, we aimed to determine the sensitivity and specificity of FST by comparing FST and caloric test results. The sensitivity and specificity of FST were found 53.3% and 78.6%, respectively. These results suggest that FST is insufficient to determine the direction and degree of peripheral vestibular pathology.Fukuda[5], in his study on 500 healthy individuals, stated that the majority of individuals retain their original positions in FST, but some individuals tend to earth-vertical axis rotation. He stated that this rotation is on the side of the slow component of spontaneous nystagmus and is caused by a tonic imbalance in the peripheral vestibular organs. He interpreted a false rotation toward the unaffected side resulting in a compensatory reflexive movement in the yaw plane toward the affected side[5]. In our study, 16 of 20 UVD patients had a correlation between the UVD direction and the FST rotation direction (rotation to the UVD side). However, there was a discrepancy between the UVD direction and FST rotation direction in 4 patients. In the literature, similar to our results, it is seen that there are some mismatches between UVD and FST[6-8]. In patients with UVD, a residual vestibular function remains similar to the residual hearing in the hearing system. This function and vestibular compensation may affect tonic imbalance, and therefore the FST rotation direction may also be affected. In addition, in the caloric test, it is generally accepted that the slow phase rate of nystagmus is more than 25% for the diagnosis of vestibular hypofunction, while lower rates of rotation in FST may explain false-negative results.
Honoker et al.[9] investigated the sensitivity and specificity of the FST in dizziness patients, similar to our study. However, unlike our study, they applied FST in two different ways; one with head shake component FST and the other as standard FST. At the end of the study, similar to our results, they stated that the standard FST had a sensitivity of 50% and a specificity of 61%, whereas the head shake FST had a sensitivity of 69% and a specificity of 39%[9]. In another study conducted by Honoker et al.[8], they divided chronic dizziness patients into 4 groups according to their caloric weakness; 0-24% unilateral weakness (normal); 25-50% unilateral weakness (mild); 51-75% unilateral weakness (moderate); 76-100% unilateral weakness. In this study, it was reported that the performance of FST was higher in patients with severe unilateral weakness[8].
In our study, we applied the FST to all patients in a silent and poorly lit vestibular test room and asked the patients to remove their shoes while performing the test. Inputs from the visual system, proprioceptive system, and vestibular system are known to have important roles in maintaining balance. Therefore, tests without shoe removal can change the proprioceptive input and affect the test result. In addition, in some recent studies, it is stated that hearing is also important for the balance system[10,11]. Therefore, applying the FST in a quiet room is important for the reliability of the test. Munnings et al.[12] investigated environmental factors affecting the FST test in normal individuals. They applied FST to individuals under different conditions. In their study, each participant was tested in both a standard clinic room and a soundproofed anechoic room under the following randomized conditions: standing on the floor, standing on foam, with or without industrial ear defenders, and in the presence or absence of a sound-localizing source[12]. As a result, they reported that environmental factors affect the test and the application of the test on foam or in a sound proofed room increases the sensitivity of the test[12]. We believe that it is important to apply FST in balance rooms away from external stimuli in order to increase sensitivity and specificity. However, despite these conditions, the sensitivity and specificity of FST were 53.3% and 78.6%, respectively. These results show us that even under optimal conditions, FST alone is insufficient to diagnose UVD. Further studies are needed to develop new modifications to increase the sensitivity and specificity of FST.
In conclusion, FST alone is insufficient to diagnose UVD for screening purposes. Therefore, other bedside tests (dynamic visual acuity, head shake, head thrust, past pointing) should be applied in addition to FST.
Reference
1) Valovich McLeod TC, Hale TD. Vestibular and balance issues following sport-related concussion. Brain Inj 2015;29(2):175-184. [ Özet ]
2) Mucha A, Collins MW, Elbin RJ, Furman JM, Troutman-Enseki C, DeWolf RM, Marchetti G, Kontos AP. A Brief Vestibular/Ocular Motor Screening (VOMS) assessment to evaluate concussions: preliminary findings. Am J Sports Med 2014;42(10):2479-8246. [ Özet ]
3) Bush ML, Bingcang CM, Chang ET, Fornwalt B, Rayle C, Gal TJ, Jones RO, Shinn JB. Hot or cold? Is monothermal caloric testing useful and cost-effective? Ann Otol Rhinol Laryngol 2013;122(6):412-6. [ Özet ]
4) Jongkees LB, Maas J, Philipszoon A. Clinical nystagmography: a detailed study of electronystagmography in 341 patients with vertigo. Pract Otorhinolaryngol (Basel) 1962;24:65-93. [ Özet ]
5) Fukuda T. The stepping test. Two phases of the labyrinthine reflex. Acta Otolaryngologica 1959;50(2):95-108. 6) Peitersen E. Vestibulospinal reflexes: alterations in the stepping test in various disorders of the inner ear and vestibular nerve. Arch Otolaryngol 1964;79:481-486. [ Özet ]
7) Peitersen E. Vestibulospinal reflexes: theoretical and clinical aspects of the stepping test. Arch Otolaryngol 1967;85:192-198. [ Özet ]
8) Honaker JA, Shepard NT. Performance of Fukuda Stepping Test as a function of the severity of caloric weakness in chronic dizzy patients. J Am Acad Audiol 2012;23(8):616-622. [ Özet ]
9) Honaker JA, Boismier TE, Shepard NP, Shepard NT. Fukuda stepping test: sensitivity and specificity. J Am Acad Audiol 2009;20(5):311-314. [ Özet ]
10) Soylemez E, Ertugrul S, Dogan E. Assessment of balance skills and falling risk in children with congenital bilateral profound sensorineural hearing loss. Int J Pediatr Otorhinolaryngol 2019;116:75-78. [ Özet ]
11) Park SH, Lee K, Lockhart T, Kim S. Effects of sound on postural stability during quiet standing. J Neuroeng. Rehabil 2011;8:67. [ Özet ]
12) Munnings A, Chisnall B, Oji S, Whittaker M, Kanegaonkar R. Environmental factors that affect the Fukuda stepping test in normal participants. J Laryngol Otol 2015;129(5):450-453. [ Özet ]