


OUTCOMES AND THE MANAGEMENT OF PERILYMPHATIC FISTULA AT TERTIARY CENTER
2Abdurrahman Yurtaslan Onkoloji Hastanesi, Nöroloji, Ankara, Turkey
Summary
The aim of this study is to better define diagnosis and management of perilymphatic fistula(PLF). This retrospective chart review from a tertiary care center is based on 43 available patient's files operated for a suspicion of PLF between 2000 and 2014. History of predisposing factors, clinical findings and investigations were documented pre- and postoperatively. Patients were divided into two groups according to intraoperative findings: group I (fistula negative) and group II (fistula positive). The evolution of symptoms showed an overall improvement of vertigo (91 %) and hearing loss (53 %) postoperatively. Audiograms showed a significant improvement postoperatively in the pure tone audiometry and bone conduction threshold of group II while group I did not show any significant improvement postoperatively in any audiogram parameter. This study failed to identify factors that could better predict the diagnosis of PLF. However, it shows that middle ear exploration with oval and round window obliteration is effective in PLF especially to decrease vestibular symptoms even when fistula is unidentified intraoperatively.Introduction
Perilymphatic fistula (PLF) remains a controversial topic and its management is still challenging. Various etiologic events have been proposed, however spontaneous PLF described in most cases are idiopathic and the etiology and pathogenesis is largely unknown.[1] Post-traumatic perilymphatic fistulas have been described following ear and temporal bone injury, particularly in the setting of temporal bone fractures.[2] The symptoms and signs of perilymphatic fistulae (PLF) are very varied and frequently misleading. There are reports of a great clinical expression variability, which makes it difficult for not only to diagnose, but also to classify or standardize its signs and symptoms.[3] It is more common to find reports of sensorineural dysacousia of varied degrees of sudden or fluctuating onset, associated with vertigo or dizziness and tinnitus. Conductive hearing loss may also occur in low frequencies.[4]The diagnosis can be suspected on the bases of the clinical and the audiometrial findings. The most common presenting symptom is senseurineural hearing loss.[5] Diagnostic methods and strategies have been reported in the literature but there is not a standard algorithm existing.[6] The most accepted diagnostic method remains intra-operative confirmation of perilymph leak at oval or round window. However, concerns have been raised regarding excessive surgical intervention given the lack of pre-operative confirmatory tests.[7]
Methods
We retrospectively evaluated the medical records of 43 patients treated for PLF suspicion with senseurineural hearing loss and/or vertigo, between 2000 and 2014. They were treated with tympanotomy and sealing of the oval and the round window membrane with or without PLF, operations were performed in the Department of Otorhinolaryngology of the University Hospital of Hacettepe. The patients ranged age from 23 to 65 years; their mean age was 44. Preoperative assessments included query of trauma history, evaluation of the spontane or induced nystagmus and pure tone audiogram (PTA). MRI was performed on some patients to detect the possible reason of sudden hearing loss such as acoustic neuroma or inner ear pathology. Once fistula test was positive and/or trauma history / high frequency hearing loss were detected, all the patients underwent surgical exploration that was carried out under general anesthesia immediately in 24 or 48 hours of initial admission. Local anesthetics was not used during the surgery for hemostasis. Sealing with connective tissue (muscle and adipose tissue) was carried out in all operated cases, even though PLF was not detected. Postoperative first day PTA was performed for measuring the bone transmission threshold of hearing and postoperative seventh day, just after removing the external ear canal packing, PTA was repeated. Informed concent for each patient and local ethic committee approval were taken for this study. For statistical analyses numerical variables were presented as mean and standard deviations, categorical variables were presented as frequencies and percents. Between-group comparisons were performed with KruskallWallis and MannWhitney U test in independent groups. Chi-Square test was used for categorical variable comparisons between independent groups. A p value lower than 0.05 was considered as statistical significance. IBM SPSS Statistics 22.0 (Chicago, IL, USA) was used for statistical analyses.Results
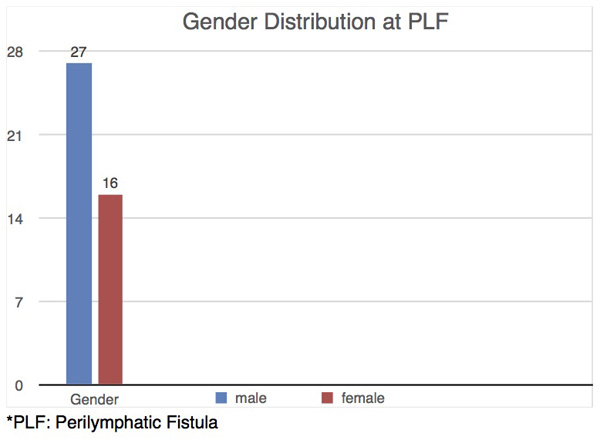
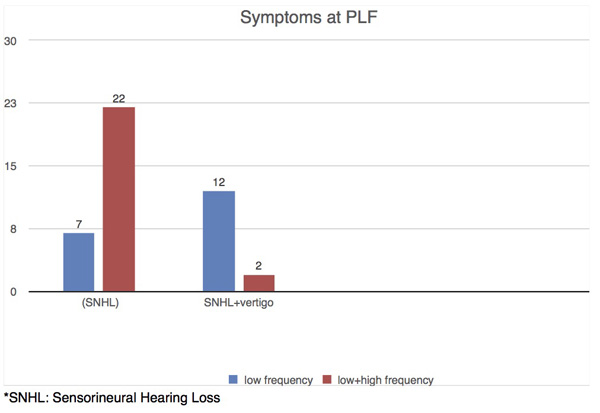
There were 27 male and 16 female patients. All of the patients had normal otoscopic findings, there were no perforation of tympanic membrane or otitis media with effusion. Thirteen patients had trauma history such as head trauma, free diving, previous surgery. Fifthteen patients had upper airway tract infection (UATI) one or two weeks before their admission. Mean follow up time is three months. Twentynine of patients complained about only SNHL, 7 of 29 patients had hearing loss affecting low frequencies, 22 of them had hearing loss which affected all frequencies and 2 of 29 patients showed nystagmus which induced by fistula test. Other 14 patients had SNHL and vertigo and 5 of them had induced nystagmus; 12 of 14 patients had hearing loss that affected especially low frequencies. None of the patients had spontane nystagmus. Table 1 summarizes all features of the patients. Systemic corticosteroid, betahistine and low molecular weight dextran were used on all of the patients. MRI was performed on 21 patients and there was no acoustic neuroma or inner ear malformations detected.){kind=link}
Table 1: Demographic features of the all patients
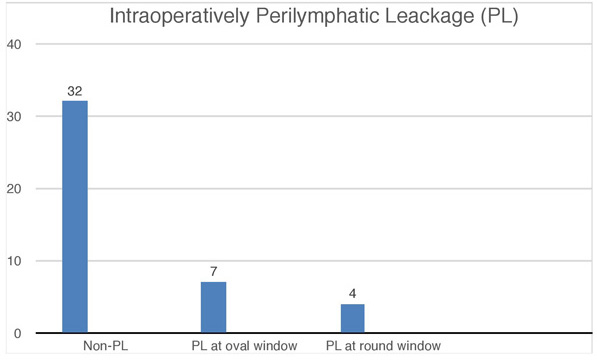
Perilymphatic leakage was not observed in 32 patients, however sealing was performed on both oval and round window (Group 1). Group 2 was consisted of 11 patients who had fistula, in 7 patients leakage was detected at oval window, in the remaining 4 cases leakage detected at round window, and sealing was carried out for both windows. Thirteen patients that 9 of them were in the group 2 showed significant improvement about their vertigo symptom up to one week after the surgery. Audiologic improvement was detected on 21 patients of whom 10 patients were in the group 2 ( 90%), when pre- and postoperative seventh day PTA were compared. Eleven of 32 patients in group 1 showed audiologic improvement (34%). Table 2 summarizes some features of the patients in group 2. In group 1, the mean hearing threshold level was 54 db before the surgery and it was 34,9 db after the surgery. In group 2, the mean hearing threshold level was 66 dB preoperatively and it was 27,6 dB postoperatively. In group 1, the avarage improvement of hearing was 19.1 dB while it was 38,4 dB in the group 2. The mean hearing threshold at admission to the hospital was 60,3 dB on the affected ear while the average improvement of hearing in all patients was 29,7 dB after the surgery (Table 3) (p<0.01). Table 2: Pre- and postoperative PTA values of the patients in group 2
){kind=link}
){kind=link}
Table 3: Hearing levels of all patients pre-and postoperatively
 Büyütmek İçin Tıklayın |
Figure 1: Demographic features of patients |
 Büyütmek İçin Tıklayın |
Figure 2: Symptomatic features of patients |
 Büyütmek İçin Tıklayın |
Figure 3: Intraoperative findings of patients |
Discussion
The treatment approach for PLF suspicion is international non-uniform and various treatment options have been proposed.[8] Tympanotomy and sealing of the round and oval window was the first indicated treatment for PLF suspicion with hearing loss and/or vertigo. However, this form of treatment has also been controversially discussed because of spontaneus recovery rate. The rate and the extent of recovery varies widely.[9] Chen et al found spontaneus remission in 31% of 52 patients with PLF suspicion, Wilson et al in 56% of 52 patients and Weinaug in 89% of 63 patients.[10,11] However, especially patients with hearing loss affecting all frequencies have a poor prognosis, regardless of the existence of vertigo. In our study no patient showed spontaneus recovery or we were not able to recognize that because all patients were treated medically and/or undergone surgery once they admitted to our clinic.Ulmulk et al evaluated the effectiveness of tympanotomy and sealing of the round window in 22 patients, 1 month after onset of hearing loss with a mean pure tone average of 67 dB before the surgery.[12] If surgery was performed within 5 days of onset of the symptoms, a significantly better mean recovery of PTA was detected. This data is consistent with the results of Reineke et al. who found a significantly better mean recovery in patients with a maximum of 8 days between onset and surgery.[13] In our study surgery was performed within 24 or 48 hours and recovery rate was filling first week after the surgery. We believe that earlier exploration provides us more satisfied results and therefore exploration should be carried out immediately in 24 or 48 hours.
The mean hearing threshold level in our study was 60,3 dB on the affected ear before the surgery and it was 30,6 dB after the surgery. The average improvement at the postoperative period was 29,7 dB. If detailing required, the avarage improvement of hearing in the group 1 was 19.1 dB while it was 38,4 dB in the group 2. It was found that complete improvement of hearing loss was detected at 17 patients and all of them had hearing loss which had affected especially low frequency. If the hearing loss affected only the low frequencies, a significantly better mean recovery of PTA was detected.
Leakage of the round window membrane occurred in 4 cases (9,3%) and 7 cases showed leakage of the oval window. However, in most of these cases (32 cases), there was no obvious leakage from the membrane but only clear fluid at the round window niche. Michel et al. reported that a b-Trace protein test had been a reliable tool to verify traces of perilymph and therefore it had been the method of choice to evaluate the existence of perilymphatic leaks.[14] We did not verify perilymphatic fluid leakage with a b-Trace test. Therefore, it is possible that the suspicious fluid noted by the operating otologist in our cases may not be of perilymphatic origin.
In group1 we did not detect the leakage however we packed the oval and round window in case of undetectable fistula. These patients might not have the fistula that's why improvement range was too low when compared with group 2. Diagnosis and treatment of PLF is still a controversial topic. Undetectable leakage was the biggest obstacle for our study. It is possible that we compared two different entities and surgical exploration could not provide us sufficient improvement for group 1. However, eventually early surgical exploration and packing must be the gold standard treatment in case of PLF suspicion.
In conclusion, tympanotomy and sealing of the oval and the round window membrane is an effective and safe method of treatment of PLF and /or PLF suspicion. Although there are some conflicts about the treatment of PLF, if the hearing loss is affecting low frequencies or it is coexisting with vertigo, the success rate of sealing is higher. If leakage was detected and sealed, the recovery of hearing could be faster and better.
Conflict of interests: No
There is no financial support or materials for this work.
Reference
1) Fukumoto I, Nemoto T, Tsukuda T, Koshizuka K. Aggravation after Diagnosis of Sudden Sensorineural Hearing Loss. Nihon Jibiinkoka Gakkai Kaiho. 2015 Mar;118(3):201-5. Japanese. [ Özet ]
2) Hoch S, Vomhof T, Teymoortash A. Critical evaluation of round window membrane sealing in the treatment of idiopathic sudden unilateral hearing loss. Clin Exp Otorhinolaryngol. 2015 Mar;8(1):20-5. doi: 10.3342/ceo.2015.8.1.20. [ Özet ]
3) Tamhankar M, Solomon D. Acute hearing loss. Curr Treat Options Neurol 2004; 6 (1) : 55–65. [ Özet ]
4) Conlin AE, Parnes LS. Treatment of sudden sensorineural hearing loss: I. A systematic review. Arch Otolaryngol Head Neck Surg 2007; 133(6):573–581. [ Özet ]
5) Cvorovic L, Deric D, Probst R, Hegemann S. Prognostic model for predicting hearing recovery in idiopathic sudden hearing loss. Otol Neurotol. 2008; 29:464–469. [ Özet ]
6) Alzahrani M, Fadous R, Dufour JJ, Saliba I. Perilymphatic fistulas: can we predict the diagnosis? Eur Arch Otorhinolaryngol. 2015 Aug;272(8):1885-91. [ Özet ]
7) Legent F, Bordure P. Perilymph fistula: myth or reality? Otorhinolaryngol Nova 1998; 8:190–196
8) Hermann M, Coelho DH. Perilymph fistula presenting with contralateral symptoms. Otol Neurotol. 2014 Feb;35(2):301-4. [ Özet ]
9) Gedlicka C, Formanek M, Ehrenberger K. Analysis of 60 Patients after tympanotomy and sealing of the round window membrane after acute unilateral sensorineural hearing loss. Am J Otolaryngol 2009; 30(3):157–161. [ Özet ]
10) Chen CY, Halpin C, Rauch SD. Oral steroid treatment of sudden sensorineural hearing loss: a ten year retrospective analysis. Otol Neurotol 2003; 24:728–733. [ Özet ]
11) Wilson WR, Byl FM, Laind N. The efficacy of steroids in the treatment of idiopathic sudden hearing loss. Arch Otolaryngol 1980; 106(12):772–776. [ Özet ]
12) Ul-Mulk J, Friis S, Hahn CH. Tympanotomy and sealing of the round window for treatment of sudden deafness. Dan Med Bul 2011; 58(5):A4276. [ Özet ]
13) Reineke U, Hühnerschulte M, Ebmeyer J, Sudhoff H. Tympanotomy and sealing of the round window membrane in sudden sensorineural hearing loss. A retrospective analysis [in German]. HNO 2013; 61(4):314-320. [ Özet ]
14) Michel O, Bamborschke S, Nekic M, Bachmann G. Beta-trace protein (prostaglandin D synthase) a stable and reliable protein in perilymph. Ger Med Sci (2005) 3:Doc04. [ Özet ]