


EAGLE SYNDROME: UNCOMMON CAUSE OF OROFACIAL PAIN; REVIEW OF 5 CASES
Summary
Eagle syndrome is an uncommon cause of orofacial pain. An elongated styloid process or calcified stylohyoid ligament triggers symptoms; most frequently as headache, facial pain, dysphagia and sensation of foreign body during swallowing. It is usually hard to diagnose if there is not enough degree of suspicion, cause the symptoms might be confused with facial neuralgias. The aim of this study is to show symptoms, steps of diagnosis and the treatment procedures of Eagle Syndrome as well as the literature review.Introduction
Patients with pharyngodynia, neck and facial pain can lead to an extensive differential diagnosis, Eagle syndrome is one of the missed out causes. Misdiagnosis and multiple failed treatments are common in certain patient population[1]. Eagle syndrome, is first described by Watt Weems Eagle in 1937, as a pair of case reports. Although etiology and pathophysiology of this syndrome was poorly understood, it was first defined as “stylalgia”and related to abnormal length of the styloid process or calcified stylohyoid membrane[2].The styloid process is a cylindrical bony projection from temporal bone. It is derived from Reichter's cartilage of the second branchial arch. Typical styloid process is about 2.5- 3.0 cm in length[3]. Lengths greater than 3 cm are considered elongated. Many important neurovascular structures lie near the tip of the styloid process. The internal carotid artery, internal jugular vein and cranial nerves X, XI, XII lie on its medial side. Compression of these structures is the main cause of the symptoms presenting. Bilateral elongation is commonly seen, but symptoms are typically unilateral.[4]
An elongated stylohyoid process occurs in about 4% of the general population as Eagle reported[5], while a small percentage of (4%-10%) the cases are symptomatic. The true incidence is about 0.16% and there is a slight female predominance[6]. Variety of symptoms in eagle syndrome is wide; such as craniofacial pain, dysphagia, odynophagia, foreign body sensation, temporary voice changes, tinnitus, otalgia, syncope and focal cerebral symptoms[7], it may also cause even stroke due to the compression of the carotid arteries and bilateral dissections of internal carotid arteries as aneurysms were described[13].
Because of the wide range of symptomes, the differential diagnosis is broad and includes glossopharyngeal neuralgia, occipital neuralgia, sphenopalatine neuralgia, temporomandibular disorders, dental infection, tonsillitis, mastoiditis, and migraine[11,12]. If appropriate clinical history and radiologic assessment is done, eagle syndrome can easily be recognized and treated.
The aim of this study is to evaluate symptoms, steps of diagnosis and the treatment procedures of Eagle Syndrome as well as the literature review.
Case Presentation
Case 1:The patient was a 68-year-old man with a-3-year history of repetitive dysphagia and left neck pain, radiating to submandibular region. He had been diagnosed with dental disease and chronic pharyngitis and was frustrated with unsuccessful treatment trials. Before admitting to our clinic, he was evaluated by a dentist and suspected about elongated styloid process after a panoramic X-ray of the jaw. His medical and surgical history was non-contributory. He did not have any craniofacial trauma either. Physical examination was performed and showed an exacerbated pain by palpation of the left tonsillar fossa. Radiographic examination demonstrated styloid process extending down (Figure 1). Elongation of the styloid process was measured as 5.39 cm. His findings were compatible with Eagle syndrome and surgical removal by transoral approach was performed. He was followed up for 4 months postoperatively, without any complaint.
 Büyütmek İçin Tıklayın |
Figure 1: Lateral cervical graphy of Case 1. It shows elongated styloid process |
Case 2:
A thirty two- year-old female patient was referred to our department with a left cervical pain, foreign body sensation in the throat and dysphagia. She also complained about a pain radiating to the left ear. In her medical history, there was not any cervical trauma or surgery. She had been medically treated by several doctors with the diagnosis of chronic pharyngitis. Through the intraoral palpation, elongated styloid process was revealed in the left tonsillar fossa, and it was painful. Lateral cervical radiography confirmed the diagnosis of Eagle syndrome, with an elongated styloid process, measured as 4.06 cm(Figure 2). Transoral removal of the styloid process was performed and a fragment of 2.1 cm was excised. The patient was asymptomatic during the following up of 3 months.
 Büyütmek İçin Tıklayın |
Figure 2: Lateral cervical graphy of Case 2. It shows elongated styloid process |
Case 3:
A 33-year-old female patient admitted to our clinic with acontinuous, daily, pressure-type pain on the right side of the neck radiating to frontal and temporal regions for 4 years. Her pain was ascending while opening her mouth. There was neither history of trauma or previous surgery, nor identifiable trigger points. Physical examination revealed pain on right tonsillar fossa with palpation, as well as on the right side of the neck. The neurological examination including the cranial nerves was normal. Towne and lateral neck radiography showed bilateral styloid process elongation (Figure 3-4). The length of the styloid processes were 5.08 cm on right and 4.7 cm on left side.She was operated by transoral approach, 1cm long styloid process removed from the right side (Figure 5).The patient was asymptomatic during the following up of 2 months.
 Büyütmek İçin Tıklayın |
Figure 3: Towne graphy of Case 3. It shows elongated styloid process |
 Büyütmek İçin Tıklayın |
Figure 4: Lateral cervical graphy of Case 3. It shows elongated styloid process |
 Büyütmek İçin Tıklayın |
Figure 5: It shows exicised styloid process |
Case 4:
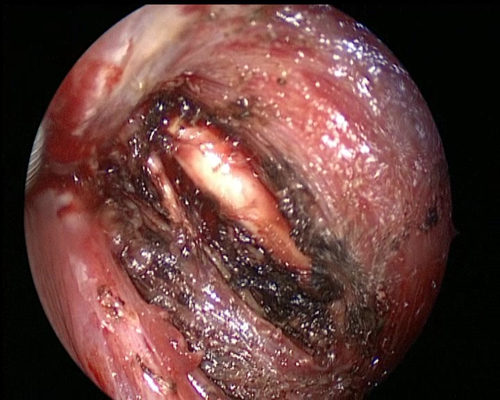
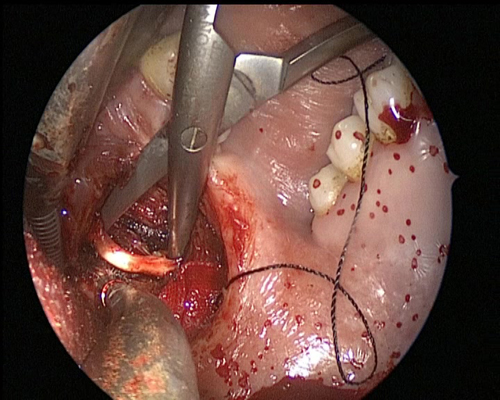
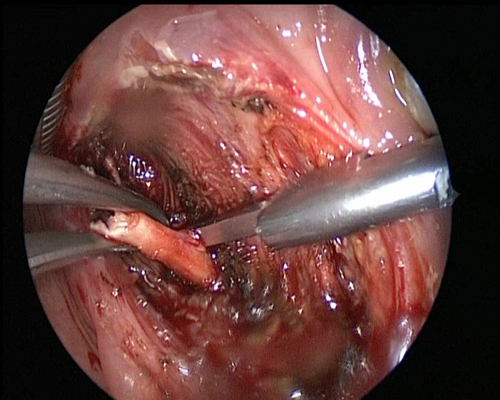
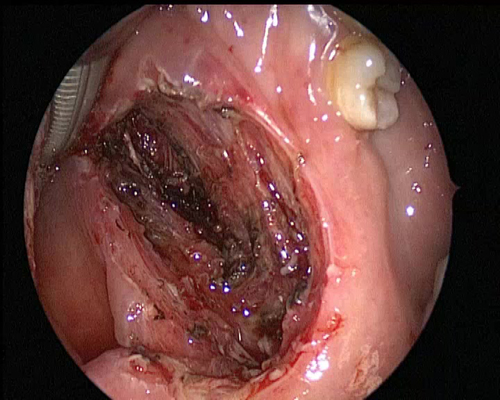
A 20-year-old female patient with repetitive dysphagia and sore throat applied our clinic. In her medical history, there was not any cervical trauma or surgery. She felt pain during the palpation of the tonsillar fossa and elongated styloid process was detected, bilaterally. Because of her pain, a neck MRI imaging was performed. Radiographic confirmed the diagnosis by showing the elongated styloid process, which was measured as 4,7cm. Transoral excision of the elongated styloid processes (bilaterally) was performed(Fig.6-9). Through the five years of follow up, she did not have pain or dysphagia.
 Büyütmek İçin Tıklayın |
Figure 6: Elongated styloid process of case 4. |
 Büyütmek İçin Tıklayın |
Figure 7: Dissection of styloid process in tonsillar fossa |
 Büyütmek İçin Tıklayın |
Figure 8: Styloid process exicion via kerrison forceps |
 Büyütmek İçin Tıklayın |
Figure 9: Parapharyngeal space after exicision |
Case 5:
The patient was a 38-year-old male with repetitive dysphagia and foreign body sensation, especially assending at night.These complaints, according to the patient, had been for 2 years. He had been administered non steroidal anti-inflammatory drugs and carbamazepine by some practitioners for facial neuralgia, without any response. Additionally, chronic pharyngitis and tonsillitis treatment had been given for many times. Elongated styloid process was revealed in the right tonsillar fossa that was tender via intraoral palpation. Styloid process elongation was detected through radiologic examination. It was measured as 5.1 cm long and excised transorally. He was followed up for four years and had never a complant again, such as repetitive dysphagia.
Methods
Five patients with elongated styloid process underwent transoral surgery in Hacettepe University, Department of Otolaryngology between 2007 and 2014. Medical records of the patients were evaluated for their age, sex, operative findings, preoperative and postoperative visuel analog scale (VAS) for pain. The duration of follow up ranged from 6 months to 7 years. Patient were underwent general physical examination. Preoperative radiologic evaluation such as Towne graphy, lateral cervical graphy, CT, panoramic X-ray was made for each patient to identify elongated styloid process. Laboratory investigations was performed and total blood count and aPTT and INR levels were evaluated, patients were asked about other systemic symptomes of inflammatory diseases and there was none. Non of the laboratory assesment was performed for the systemic inflammatory diseases, that results in cartilage and bone distruction (such as Rheumatoid arthritis and Ankylosing spondylitis), because of the lack of systemic symptomes. All patients operated transoral approach. Informed consept was taken from each patient. None of them had any complications such as airway edema or retropharyngeal infection After surgical exicion of styloid process cases were hospitalized for two days to observe the airway and there was not any sign of respiratory distress. All cases were given intravenous antibiotic therapy during hospitalization and after discharge oral antibiotic treatment was continued for 10 days. After begining this study procedure, the patients were asked to evaluate their preoperative and postoperative symptoms. They were instructed to rate their symptoms severity, by using a visual analog scale (VAS). The patients were talled that, according to VAS , (-) means no symptom, (+) referes mild symptom, (++);moderate severity, and (+++) referes severe degree of symptom. Preoperative and postoperative results of VAS, are shown on Table 1. As seen on the table 1, symptoms seen among our patients were dysphagia, orofasial pain, foreign body sensation. Among our patients; temporary voice changes, tinnitus, syncope and focal cerebral symptom did not occur. When estimated, all patients primary symptom was defined as being “severe”. The dominant symptom seen between our patients was dysphagia, and it was seen that all the symptoms were releaved after surgical treatment.){kind=link}
Table 1: Comparison of preoperative and postoperative symptom severity scores.
Discussion
The “classical Eagle syndrome” is typically seen in patients after pharyngeal trauma or tonsillectomy, and it is characterized by ipsilateral dull and persistent pharyngeal pain, centered in the ipsilateral tonsillar fossa, that can be referred to the ear and exacerbated by rotation of the head. A mass or bulge may be palpated in the ipsilateral tonsillar fossa and the palpation can also exacerbate patient's symptoms[7,8]. The “second form” of the syndrome (“stylocarotid syndrome”) is characterized by the compression of the internal or external carotid artery (with their peri-vascular sympathetic fibers) by a laterally or medially deviated styloid process[9]. It is related to a pain along the distribution of the artery, which is provoked by rotation and compression of the neck. It's not related with tonsillectomy. In case of impingement of the internal carotid artery, patients often complain about supraorbital pain and parietal headache. In case of the external carotid artery irritation, the pain radiates to the infraorbital region[10].While evaluating the patient, history of symptoms should be taken carefully. Three main criteria have generally proposed for clinical diagnosis: a characteristic dull, nagging pain that is provoked during swallowing, a palpable elongated styloid process in the tonsillar fossa, and detection of a process 30 mm or longer on radiologic evaluation.
Diagnosis is classically based on the clinical signs and palpation of the styloid process in the tonsillar fossa. Radiological findings and pain loss after local anesthetic (lidocain test) infiltration can also support the diagnosis. Lidocain test was described as local injection of 1mL of 2% lidocaine into tonsillar fossa. Following the injection pain relives and it can be used as a diagnostic test for elongated styloid process[14]. Panoramic radiographs, Towne graphs and lateral cervical graphs can be performed to see the elongated styloid process. Computerized tomography (CT) is to be considered the gold standard for diagnosis[15] when it is performed three-dimensional. 3D-CT is a valuable diagnostic tool in the diagnosis of Eagle's syndrome because of its ability to facilitate accurate measurement of the length of the styloid process[16,17].
Treatment can be surgical and non-surgical. Non-surgical approaches consist of using non-steroidal anti-inflammatory medications, oral neuro-protective agents such as gabapentin, amitriptyline, valproate, carbamazepine and infiltration of steroids or anesthetics in the tonsillar fossa[18]. Surgical excision of the elongated styloid process with the external approach (transcervical) or transoral (transpharyngeal) approaches are often preferred[19]. As an otolaryngologist, we almost often perform the transoral approach. Through an oral corridor, afterwards tonsillectomy, an incision is made anterior to the tonsillar fossa and the tip of the styloid process is exposed via blunt dissection (Figure 6). This dissection is proceeded as proximally as possible along the styloid process, ultimately leading to removal of the process at the base (Figure 7). Complete exposure and thus complete excision of the styloid process are often not possible with this approach, although the excised component is almost always sufficient to relieve symptoms (Figure 8 and 9). The transoral approach is favored for its cosmetic by avoiding any external incision and for it's potential for shorter operation time[20,21]. Nevertheless, exposure of the retropharyngeal space to intraoral contents elevates the risk of infection. Further considerations include poor carotid artery access in case of intraoperative injury[22], airway edema, and trismus . In case of the elevated risk of airway edema, bilateral operations must be staged[20].
In the external approach, an oblique incision is made in the skin crease halfway between the angle of the mandible and the tip of the mastoid process. Dissection begins with opening of the superficial fascia and posterolateral retraction of the sternocleidomastoid muscle. With ongoing blunt dissection, superior retraction of the parotid gland, inferior retraction of the posterior belly of the digastric muscle, identification and preservation of the facial vein can be achieved. The elongated styloid process is identified and detached from the stylohyoid ligament distally. Muscular attachments are removed via subperiosteal dissection. The styloid process is then removed completely in a piecemeal fashion[23]. The operating surgeon should take care to expose and then to avoid the mandibular branch of the facial nerve in the superficial fascia as well as external carotid artery branches within the deep fascia. The most common postoperative complication of the external approach is weakness of the mandibular branch of the facial nerve, which is usually transient. The primary advantage of this approach is the minimal generation of airway edema, and the consequent ability to perform bilateral styloidectomyin the same session. Minimally invasive external approaches involving styloid chain transection and resection of the lesser cornu of the hyoid bone have been used with the aid of stereotactic navigation. These approaches are rare, and there is not yet a consensus about their utility[24].
Conclusion
Although eagle syndrome's symptoms are similar to other pathologies and it creates a complex and difficult condition to diagnose. Physical examination and radiological evaluation are supportive to make the diagnosis. Eagle syndrome can be successfully treated with surgery and in most of the cases, pain relief can be provided. A surgical exicion of this elongated styloid process is the main treatment option and transoral approach has lesser complication incidence.Reference
1) Zeckler, S.R., A.G. Betancur, and G. Yaniv, The eagle is landing: Eagle syndrome--an important differential diagnosis. Br J Gen Pract, 2012. 62(602): p. 501-2. [ Özet ]
2) Blackett, J.W., et al., Trigeminal neuralgia post-styloidectomy in Eagle syndrome: a case report. J Med Case Rep, 2012. 6(1): p. 333. [ Özet ]
3) Ferreira, P.C., et al., Eagle syndrome. J Craniofac Surg, 2014. 25(1): p. e84-6. [ Özet ]
4) Jewett, J. and R. Moriarity, Eagle syndrome: an incidental finding in a trauma patient: a case report. J Emerg Med, 2014. 46(1): p. e9-e12. [ Özet ]
5) Uludag, I.F., et al., Eagle syndrome: case report. Agri, 2013. 25(2): p. 87-9. [ Özet ]
6) Demeter, M., et al., Eagle syndrome. JBR-BTR, 2013. 96(1): p. 48. [ Özet ]
7) Kumar, P., A.P. Rayamane, and M. Subbaramaiah, Sudden death due to eagle syndrome: a case report. Am J Forensic Med Pathol, 2013. 34(3): p. 231-3. [ Özet ]
8) Yildiray, S., et al., A patient with Eagle syndrome: radiological and scintigraphic evaluation. Indian J Dent Res, 2012. 23(2): p. 283-5. [ Özet ]
9) Todo, T., et al., Eagle syndrome revisited: cerebrovascular complications. Ann Vasc Surg, 2012. 26(5): p. 729 e1-5. [ Özet ]
10) Texier, C., et al., Eagle syndrome, a rare cause of glossodynia. Eur J Dermatol, 2012. 22(5): p. 702-3. [ Özet ]
11) Lonka, M.M. and L.P. Schousboe, [Unilateral atypical neck pain in Eagle syndrome]. Ugeskr Laeger, 2012. 174(18): p. 1242-3. [ Özet ]
12) Alves, N.D. and M. Sousa, [Eagle syndrome]. Acta Med Port, 2012. 25(5): p. 348. [ Özet ]
13) Cano, L.M., P. Cardona, and F. Rubio, [Eagle syndrome and carotid dissection]. Neurologia, 2010. 25(4): p. 266-7. [ Özet ]
14) Kim, E., K. Hansen, and J. Frizzi, Eagle syndrome: case report and review of the literature. Ear Nose Throat J, 2008. 87(11): p. 631-3. [ Özet ]
15) Murtagh, R.D., J.T. Caracciolo, and G. Fernandez, CT findings associated with Eagle syndrome. AJNR Am J Neuroradiol, 2001. 22(7): p. 1401-2. [ Özet ]
16) Way, T.J., P.M. Weinberger, and B.J. McKinnon, Radiology quiz case 2. Eagle syndrome. Arch Otolaryngol Head Neck Surg, 2009. 135(8): p. 829. [ Özet ]
17) Karam, C. and S. Koussa, [Eagle syndrome: the role of CT scan with 3D reconstructions]. J Neuroradiol, 2007. 34(5): p. 344-5. [ Özet ]
18) Nickel, J., et al., [Eagle syndrome: diagnostic imaging and therapy]. Rontgenpraxis, 2003. 55(3): p. 108-13. [ Özet ]
19) Slavin, K.V., Eagle syndrome: entrapment of the glossopharyngeal nerve? Case report and review of the literature. J Neurosurg, 2002. 97(1): p. 216-8. [ Özet ]
20) de Souza Carvalho, A.C., et al., Intraoral approach for surgical treatment of Eagle syndrome. Br J Oral Maxillofac Surg, 2009. 47(2): p. 153-4. [ Özet ]
21) Leclerc, J.E., Eagle syndrome: teaching the intraoral surgical approach with a 30 degrees endoscope. J Otolaryngol Head Neck Surg, 2008. 37(5): p. 727-9. [ Özet ]
22) Farhat, H.I., et al., Eagle syndrome as a cause of transient ischemic attacks. J Neurosurg, 2009. 110(1): p. 90-3. [ Özet ]
23) Martin, T.J., D.R. Friedland, and A.L. Merati, Transcervical resection of the styloid process in Eagle syndrome. Ear Nose Throat J, 2008. 87(7): p. 399-401. [ Özet ]
24) Rezgui-Marhoul, L., et al., [Eagle syndrome: case report]. Rev Stomatol Chir Maxillofac, 2004. 105(1): p. 50-2. [ Özet ]